Fig. 4.1
(a, b) Normal pancreatic duct epithelium. (b) A magnified image. Epithelial lining composed of a single layer of cuboidal cells
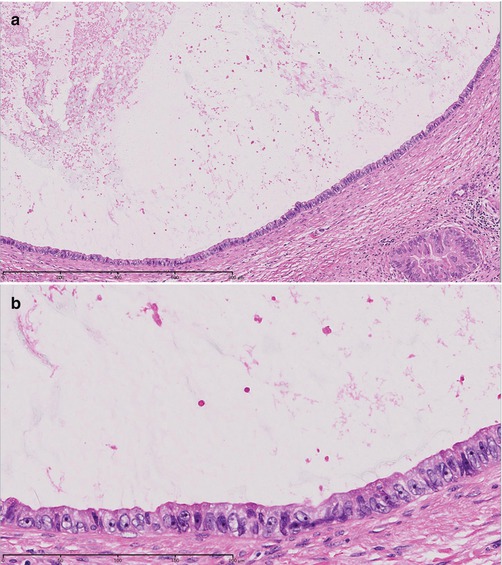
Fig. 4.2
(a) Carcinoma in situ composed of a single cell layer. (b) A magnified image. Epithelial lining composed of a single layer of cuboidal cells. The case was diagnosed as carcinoma in situ, because the cells composing the epithelium are larger in size than those shown in Fig. 4.1a. The normal epithelial cell count (Fig. 4.1b) is about 20 cells/100 μm. However, the epithelial cell count in this image is about 10 cells/100 μm, with the cell size being about twofold larger. The nuclear shape is irregular
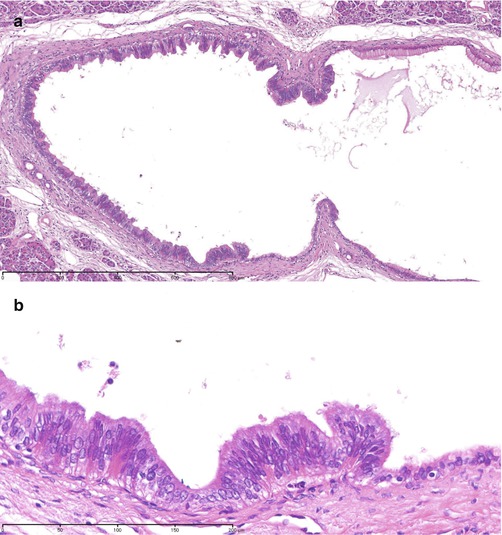
Fig. 4.3
(a) Carcinoma in situ in a single layer of tall columnar cells. (b) The cells have spindle-shaped nuclei and show milder nuclear atypia than that observed in Fig. 4.2. However, the case was diagnosed as carcinoma in situ based on the following findings: a clear border was seen between the nonneoplastic epithelium and atypical cells, and the cell density was high, with the nuclei located away from the base of the cells and spaced irregularly
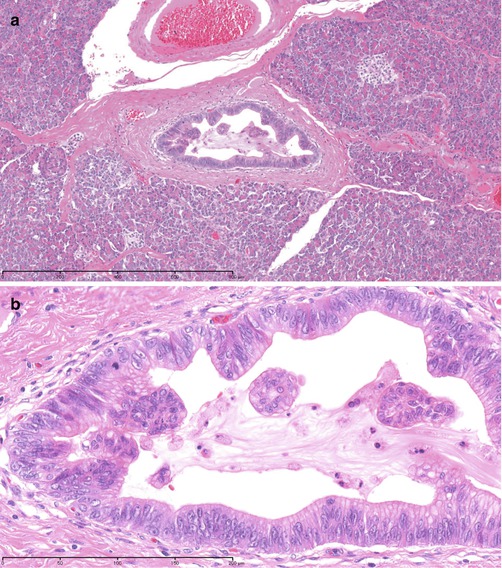
Fig. 4.4
(a) Carcinoma in situ in a single layer of cells, partly showing low-papillary growth. (b) It is difficult to differentiate between carcinoma and epithelium with atypia, because in a single layer of cells, the cells are relatively small in size and show less severe atypia. The area showing papillary growth was diagnosed as carcinoma based on the presence of cellular and structural atypia. Since the cells in the single cell layer are similar to the cells in the area showing papillary growth, the lesion was diagnosed as carcinoma in situ
Fig. 4.5
(a, b) Epithelial mucous cell hyperplasia. Cells in mucous cell hyperplasia show a high frequency of point mutations in the Ki-ras oncogene and therefore are determined to be neoplastic by genetic analysis. However, clinically, even over long-term observation, these cells remain unchanged in morphology, being neither invasive nor metastatic. Therefore, histopathologically, such cells are diagnosed as mucous cell hyperplasia, which is regarded as a benign lesion
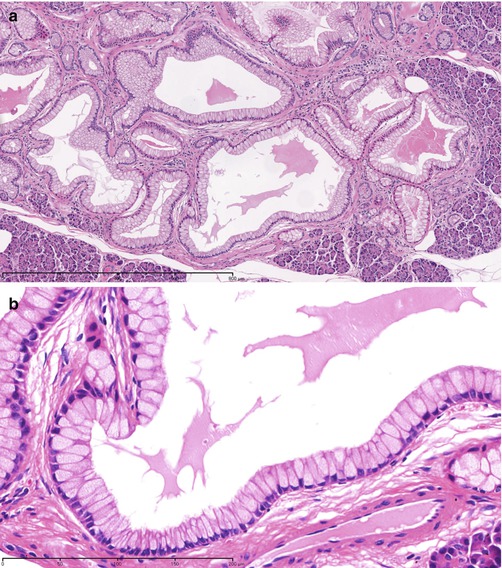
Fig. 4.6
(a) Glandular hyperplasia: proliferation of glandular ducts composed of epithelial mucous cell hyperplasia. (b) Proliferation of glandular ducts composed of cells similar to those shown in Fig. 4.5 is observed
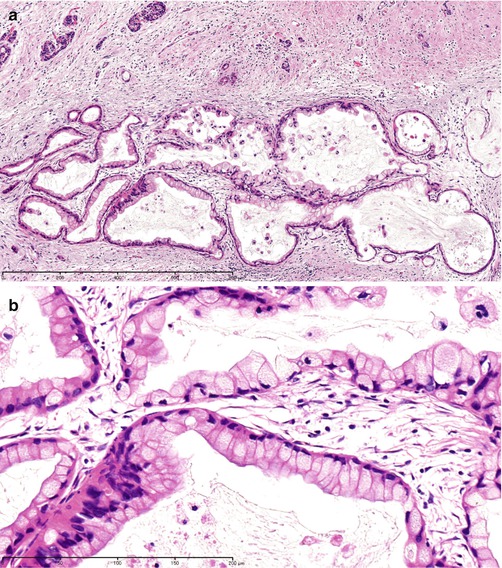
Fig. 4.7
 Staging and Determination of Resectability of Pancreatic Cancer
Laparoscopic Distal Pancreatectomy in Pancreatic Cancer
Staging and Determination of Resectability of Pancreatic Cancer
Laparoscopic Distal Pancreatectomy in Pancreatic Cancer
 PET and Other Functional Imaging
PET and Other Functional Imaging
 Mesenteric Approach for Pancreaticoduodenectomy
Mesenteric Approach for Pancreaticoduodenectomy
 Role of Extended Resection in Pancreatic Cancer
Role of Extended Resection in Pancreatic Cancer
 Emerging New Treatment Modalities: Irreversible Electroporation
Emerging New Treatment Modalities: Irreversible Electroporation




(a) Carcinoma in situ showing proliferation of glandular ducts composed of cells containing abundant mucus in the cytoplasm, similar to the cells shown in Fig. 4.6. (b) Proliferation of glandular ducts composed of a single layer of cells containing abundant mucus in the cytoplasm is observed, as shown in Figs. 4.5 and 4.6. The lesion was diagnosed as carcinoma in situ, because the sizes of the cells composing the glandular epithelium are not uniform, and the nuclei are spaced irregularly, as compared to the regularly spaced nuclei located in the basal portion of the cells shown in Figs. 4.5 and 4.6
Related posts:
Staging and Determination of Resectability of Pancreatic Cancer
Laparoscopic Distal Pancreatectomy in Pancreatic Cancer
PET and Other Functional Imaging
Mesenteric Approach for Pancreaticoduodenectomy
Role of Extended Resection in Pancreatic Cancer
Emerging New Treatment Modalities: Irreversible Electroporation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
