Chapter 10 CONSULTATION–LIAISON SERVICES TO RESIDENTIAL AGED CARE FACILITIES
INTRODUCTION
Community mental health teams for older people often provide consultation–liaison services to residential aged care facilities (RACFs). A consultation–liaison service has two components:
RESIDENTIAL AGED CARE
In 2008, Australia had 175,472 places in 2830 RACFs, with an average of 57 places per facility (Australian Institute of Health and Welfare 2009). These places cater for people who are deemed to have low-care and high-care needs. Traditionally, RACFs were staffed and designed to deal with residents with chronic physical disabilities, rather than mental health problems. However, two factors have combined to generate a need for mental health consultation–liaison services. Firstly, the proportion of residents with dementia and associated psychological and behavioural problems has risen dramatically in the past two decades. Secondly, many older people with mental health problems were transferred to RACFs during the deinstitutionalisation of large mental institutions.
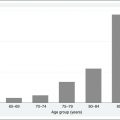
Estimates of the prevalence of mental health problems in RACFs have been subject to several studies. Brodaty et al (2001), in a study of 11 Sydney (Australia) nursing homes involving 647 residents using the BEHAVE–AD scale, established prevalence rates for the behavioural and psychological symptoms of dementia (BPSD), psychosis, depressed mood, activity disturbance and aggression (see Table 10.1). Neville and Byrne (2007), using the Dementia Behavior Disturbance Scale (DBDS), found that 89% of older people in residential respite care displayed one or more BPSD, although not necessarily all the time. The prevalence of all types of dementia was rated at 48% by the Australian Institute of Health and Welfare (2006); however, other studies have estimated that dementia can affect up to 90% of older people in residential care (Rosewarne et al 1997). A North American study found a 40% prevalence rate for anxiety in older people in RACFs (Larson & Lyons 1994). Despite these high rates, mental health problems are poorly recognised and treated in RACFs. When treatment is provided, it often consists solely of psychotropic medication prescribed by a general medical practitioner (Shea et al 1994).
Table 10.1 Prevalence rates of mental health problems in RACFs
| Mental Health Problem | Prevalence Rate |
|---|---|
| BPSD (at least one symptom) | 89% |
| Psychosis | 60% |
| Depressed mood | 42% |
| Activity disturbances/aggression | 82% |
| Dementia (all types) | 48–90% |
| Anxiety | 40% |
Source: Brodaty et al (2001), Larson and Lyons (1994), Neville and Byrne (2007) and Rosewarne et al (1997).
Providing consultation–liaison in an RACF environment can be challenging for the mental health worker, as there are a number of potential barriers to be overcome (Craig & Pham 2006). These barriers include high staff turnover and clinical staff who are unlicensed or have limited education or training in mental health problems leading to poor understanding of symptoms and poor attitudes to mental health problems (Hsu et al 2005). This lack of understanding of mental health problems can also extend to visiting medical practitioners. In addition, financial constraints and staff recruitment issues may result in minimal staffing levels where only the basic physical needs of the residents are able to be met. Staff can also be concerned about accepting new services for fear of exposure of other problems that cannot easily be solved (Tourigny-Rivard & Drury 1987).
The consultation–liaison role involves working at the relationship with the older person, their family and the personnel involved in their care. The benefits of this approach have been found to include better diagnosis and management of a range of mental health problems, identification of medication problems, improved tolerance of behavioural symptoms, increased use of new interventions and a reduction in hospital admissions (Fuller & Lillquist 1995, Goldman & Klugman 1990).
THE CONSULTATION–LIAISON PROCESS
The majority of consultation–liaison services are for assessment and treatment of behavioural symptoms (e.g. pacing and wandering, verbal abusiveness and disruptive vocalisations, physical aggression and resisting care). Kat et al (2008) examined reasons for consultation referrals in Dutch nursing home residents with dementia. Common reasons for referral included agitation, disinhibition and aberrant motor behaviour. These researchers noted their surprise that delusions, irritability and eating behaviour changes were not more common, considering the reasonably high prevalence rates of these symptoms that usually occur in this population. Conspicuous by their absence were common abnormal behaviours such as apathy, which are often considered less troubling to RACF staff.
The consultation–liaison process is complex and involves getting to know the working culture of the RACF, as many personnel as possible (clinical, administrative and domestic) and the major sources of referral. Initially, certain elements of this process have to be clarified (e.g. who the target for intervention is). It could be the system, the resident, the staff members or perhaps even family members if they are heavily involved in the care of the older person. Some family members experience persisting grief and remain devoted to the care of the older person even after permanent admission. They sometimes spend many hours every day of the week in attendance. The intervention may be delivered directly to the older person or indirectly through working with staff and relatives. Sometimes, if the problem is a systemic one (i.e. it is occurring frequently in a number of people), the level that may need to be addressed could be the facility management so that policies and procedures are modified to resolve the problem. A good guide on how to undertake the consultation process has been provided by Caplan (1970), and it can be easily applied to the consultation–liaison role. The steps are:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


