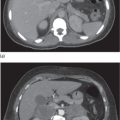
Boys may develop testicular masses (‘adrenal rests’) due to ectopic adrenal cells stimulated by ACTH hypersecretion. They are typically bilateral and may be diagnosed as early as 5 years, but usually present between the ages of 10 and 20 years (see ‘Presentations in adolescents and adults’ below).
Classic simple virilizing
In this form of CAH, aldosterone secretion is adequate, but cortisol is not synthesized efficiently.
Girls present with ambiguous genitalia (see above).
Boys present at 2–4 years of age with early virilization and signs of puberty (pubic hair, growth spurt, adult body odour). Boys may also develop testicular adrenal rests (see below).
Presentations in adolescents and adulthood
Reproduction
In females, fertility rates may be reduced by hyperandrogenaemia due to inadequate glucocorticoid therapy (resulting in menstrual irregularity) and/or structural abnormalities due to androgen excess in utero or suboptimal surgical reconstruction. In women with simple virilizing and salt-losing CAH, respective fertility rates of up to 80% and up to 60% may be achieved with treatment.
In males, high levels of adrenal androgens (if poorly controlled) suppress gonadotrophins and therefore testicular function and spermatogenesis. Boys or young men may develop testicular masses composed of ectopic adrenal tissue (‘adrenal rests’) that is stimulated by the increased ACTH. They are more common in the salt-losing form as they tend to have poorer control and higher ACTH levels. They are benign but may lead to obstruction of the seminiferous tubules, gonadal dysfunction and infertility.
Stature
Exposure to high levels of sex hormones leads to accelerated growth in childhood but induces premature epiphyseal closure, resulting in a short final adult stature. Excess glucocorticoid therapy may also suppress growth and contribute to adult short stature.
Non-classic CAH (late-onset)
Non-classic or late-onset CAH may present as hirsutism, acne and menstrual irregularity in young women, and early pubarche or sexual precocity in school-age children, or there may be no symptoms.
Rarer forms of CAH
11 β-Hydroxylase deficiency
Increased deoxycorticosterone (Fig. 9.1) (which has mineralocorticoid activity) results in hypertension and frequently hypokalaemia. Increased androgens result in the virilization of female foetuses, causing ambiguous genitalia (female pseudohermaphrodism).
3 β-Hydroxysteroid dehydrogenase deficiency
Mineralocorticoid (Fig. 9.1) deficiency results in salt wasting and hyperkalaemia. Reduced androgens in men result in ambiguous genitalia (male pseudohermaphrodism) ranging from hypospadias to nearly normal female external genitalia. Increased dehydroepiandrosterone (DHEA) in women may result in a mild virilization of the external genitalia.
17 α-Hydroxylase deficiency
Increased mineralocorticoids (Fig. 9.1) result in hypertension and frequently hypokalaemia. Reduced adrenal and gonadal sex steroids result in ambiguous genitalia in men (male pseudohermaphrodism), with a blind vagina, no uterus or fallopian tubes, intra-abdominal testes and absent puberty/primary amenorrhoea in females.
Investigations
Classic CAH
Most patients with classic CAH are diagnosed in infancy. An elevated level of 17-hydroxyprogesterone indicates 21-hydroxylase deficiency. 17-Hydroxyprogesterone is a precursor steroid that accumulates upstream of the enzyme defect (see ‘Aetiology’). However, the test should be repeated (along with 11-deoxycortisol measurement) after 48 hours of age to distinguish CAH from the physiological hormonal surge in the first 2 days of life. Hyponatraemia and hyperkalaemia indicate a salt-losing crisis. Plasma renin level is useful in confirming salt wasting.
Genetic analysis may be performed to identify specific CYP21 mutations.
In infants with ambiguous genitalia, karyotyping and gender assignment should be done urgently. The initial evaluation should include ultrasonography of the internal genitalia (uterus).
Because of the high prevalence of testicular adrenal rests and their association with infertility in male patients, they should be monitored by testicular ultrasonography in adolescence or early adulthood.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


