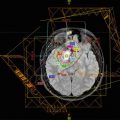
Fig. 25.1
A non-coplanar 3DCRT plan on left shows a less conformal prescription dose distribution around the concave PTV in red. An IMRT plan is more conformal around the PTV with more brain receiving a low dose
The understanding of SMN risk after is limited as many reports have small numbers from single institutions or have limited follow-up of modern techniques. Various mathematical models exist for estimating SMN and a large part of our understanding stems from estimated total body doses to survivors of the atomic bomb and other organ-specific models have been proposed. The calculated risk of SMN of fixed beam IMRT vs. VMAT in the medium to high-dose region exceeding 2.5 Gy is approximately equal (Moteabbed et al. 2014). There is no threshold radiation dose for SMN development. In other words, any tissue receiving any radiation could in theory develop an SMN.
Comparable tumor coverage can be achieved with both 3D and IMRT techniques. Reports comparing the two techniques bear this out although the long-term follow up is generally longer in 3DCRT making such comparisons more challenging. The proliferation of IMRT delivery has also accompanied technological advancements in 6D treatment couches, image-guidance, and thermoplastic immobilization devices, all of which has made more conformal treatment with minimal intra-fractional variability possible (Lightstone et al. 2012). Although dosimetric comparisons between 3D and various IMRT techniques have long been possible, there are fewer publications detailing long-term clinical outcomes of pediatric CNS malignancies treated with IMRT. Low grade glioma (LGG) represents a heterogeneous subset of pediatric CNS tumors in terms of pathology and prior therapies before radiation. Patterns of recurrence using IMRT techniques including simultaneous integrated boost do not differ from 3DCRT. Most recurrences occur in the primary tumor volume (Paulino et al. 2013). Hippocampal sparing VMAT dosimetry has been described (Kazda et al. 2015). Regardless of radiation technique a primary determinant of neurocognitive effects, as well as recurrence, is age at the time of treatment (Merchant et al. 2009; Oh et al. 2011; Paulino et al. 2013). Similarly for ependymoma and craniopharyngioma the utilization of 3DCRT versus IMRT does not impact recurrence (Merchant et al. 2006, 2013; Schroeder et al. 2008; Greenfield et al. 2015).
Estimates of different long-term toxicities based on dosimetric data are speculative but possible. CNS germinoma has an excellent prognosis. For whole ventricular RT (WVRT), IMRT spares normal brain better than 3DCRT for which the fields are opposed laterals (Chen et al. 2010). Estimates of the 5-year effect of either 3DCRT or VMAT on IQ of patients with CNS germinoma receiving WVRT 23.4 Gy followed by a boost to 21.6 Gy have been calculated. The VMAT plan had better a CI with only a slightly higher HI. Due to improved conformity and less to the temporal lobes, the projected IQ of the VMAT patients was higher than 3DCRT (Qi et al. 2012).
The superior conformity of IMRT over 3DCRT after craniospinal axis irradiation (CSI) is evident when comparing boost plans covering the posterior fossa (PF) for medulloblastoma. 3DCRT covering the PF with opposed fields covering 90% of the cochlea with the prescription dose while covering 50% of the pituitary gland with 80% of the prescription dose. IMRT can reduce the 90% coverage of the cochlea to 33.4% while reducing the 50% coverage of the pituitary to 20% of the PF prescription dose (St Clair et al. 2004). For treatment of the resection cavity plus margin for medulloblastoma, the CI of IMRT is superior to 3DCRT without an increase in recurrence. 3D conformal radiation and IMRT allowed for a limited volume of the posterior fossa to be covered, making radiation to the resection cavity plus margin an option. Both approaches offering sparing of critical structures compared to 2D radiation of opposed laterals using bony anatomy to define the posterior fossa. A three-dimensional beam arrangement utilizing oblique coplanar wedged pair can offer similar coverage to the posterior fossa while sparing the cochlea and pituitary gland at the cost of a higher dose to the thyroid than opposed laterals (Tarbell et al. 2000).
The group from Memorial Sloan Kettering has published their experience using fixed beam IMRT to treat IFRT for the boost after CSI. In this series, there were no isolated posterior fossa recurrences outside of the boost volume. Treating the resection cavity plus a margin was effective with no recurrences in 10 patients with a median follow-up of 42 months in a report from Memorial Sloan Kettering (Merchant et al. 1999). The authors describe six combinations of gantry and couch positions for a midline tumor. Patients did receive cisplatin-based chemotherapy but the short-term ototoxicity compared favorably to other reports (Polkinghorn et al. 2011). The group from Baylor utilized IMRT for IFRT boost and compared the dosimetry and toxicity to a cohort treated with 3DCRT. All patients were in the pediatric age group and received chemotherapy. Despite receiving more cisplatinum, the patients treated with IMRT had a lower rate of hearing loss: 13% Grade 3 or 4 versus 64% in the conventional RT group (p < 0.014). Forty-seven percent of the IMRT group had no hearing loss (Huang et al. 2002).
A variety of techniques have been utilized for craniospinal radiation. Prone treatment allows for easily visualization of the SSD skin marking but adds to the difficulty with the changing geometry of couch rotations for the spinal fields and collimator rotation for the cranial field, particularly in patients who are undergoing anesthesia. Common practice today is supine treatment for craniospinal axis radiation. Photon CSI is now done with 3D planning a minimum. IMRT can be done for the entire volume or in conjunction with 3DCRT. A standard 3D approach includes choosing spine isocenters at fixed distances from the brain field isocenter, then shifting the asymmetric jaws to “feather the gap” at matched fields (Parker and Freeman 2006). IMRT can be used in an otherwise 3D plan to match the fields over several centimeters, allowing for one CSI plan as opposed to generating multiple 3D plans at different match lines. Helical tomotherapy has the advantage that the entire craniospinal volume in a single uninterrupted field (Fenwick et al. 2006). Intensity-modulated radiation can improve the conformity of a craniospinal radiation plan but has a higher integral dose than a 3D plan (Mascarin et al. 2011; Harron and Lewis 2012).
VMAT for the spinal portion of CSI offers several dosimetric advantages of a standard 3DCRT plan with a single poster field on the spine including more conformity with less heterogeneity in the target volume. VMAT can give a lower mean cardiac dose, while giving a higher mean lung dose with a smaller percentage of the lung receiving higher doses above 20 Gy for a prescription dose of 23.4 Gy (Lee et al. 2012). Despite the entire lungs receiving some “low dose bath” from VMAT CSI with concurrent chemotherapy, acute radiation pneumonitis is rare (Penagaricano et al. 2009). An alternative to straight posterior beam to cover the spine is a 3-field approach. A 3D-CRT 3-field plan using a straight posterior two posterior oblique fields compares favorable to VMAT when comparing heart dose, while giving slightly more dose to the kidneys, and distributing more high dose but less low dose to the lungs (Bandurska-Luque et al. 2015).
Photon radiation is commonly utilized for the treatment of pediatric brain tumors and has the most long-term published data on tumor control and side effects. The decision to utilize IMRT or 3DCRT depends on many factors. Dose conformity is superior to IMRT at the cost of slightly higher heterogeneity and increased integral dose. When deciding between 3DCRT and IMRT, the treating radiation oncology must consider the benefits of conformity versus the potential long-term effects of low doses to organs at risk. Our understanding of the long-term toxicities of radiation for pediatric CNS malignancies continues to evolve as the relationship between radiation dose and critical normal structures including the hippocampus continues to expand.
References
Bakiu E et al (2013) Comparison of 3D CRT and IMRT treatment plans. Acta Inform Med 21(3):211–212CrossrefPubMedPubMedCentral
Bandurska-Luque A et al (2015) Prospective study on dosimetric comparison of helical tomotherapy and 3DCRT for craniospinal irradiation—a single institution experience. Rep Pract Oncol Radiother 20(2):145–152CrossrefPubMedPubMedCentral
Related posts:
 Chemotherapeutic Strategies in Brain Tumors
Chemotherapeutic Strategies in Brain Tumors
 Neuropsychological Late Effects of Radiotherapy for Pediatric Brain Tumors
Neuropsychological Late Effects of Radiotherapy for Pediatric Brain Tumors
 Atypical Teratoid Rhabdoid Tumors (AT/RT) and ETMR
Atypical Teratoid Rhabdoid Tumors (AT/RT) and ETMR
 Low-Grade Glioma
Low-Grade Glioma
 Proton Therapy for Skull Base Chordomas in the Pediatric and Adolescent Patient
Proton Therapy for Skull Base Chordomas in the Pediatric and Adolescent Patient
 Second Neoplasms After Successful Treatment for Pediatric Central Nervous System Tumors
Second Neoplasms After Successful Treatment for Pediatric Central Nervous System Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


