Fig. 20.1
Pancreatic blood supply. IPDA inferior pancreaticoduodenal artery, GDA gastroduodenal artery, SA splenic artery
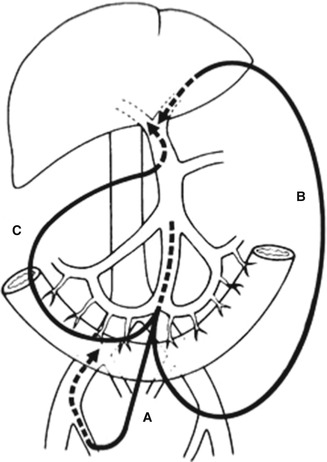
Fig. 20.2
Catheter bypass of the portal vein: (A) bypass between the mesenteric and femoral veins, (B) bypass between the mesenteric and umbilical veins, (C) bypass between the mesenteric and hepatic hilar portal veins (From reference No. [5])
In cancer surgery, “isolated” means en bloc resection using a non-touch isolation technique. Before manipulation of the pancreatic head cancer, all arteries that supply the pancreatic head region and all drainage veins for this region are ligated and divided (Fig. 20.1). Our first step in performing the PD is a mesenteric approach; we do not perform Kocher’s maneuver. This mesenteric approach involves clearing the connective tissue around the SMV and superior mesenteric artery (SMA) in the mesenteric root, which includes systematic lymphadenectomy around the SMA [17]. Resection starts from the non-cancerous side and cancer-free surgical margins, and resectability can be diagnosed before proceeding. The inferior pancreaticoduodenal artery (IPDA) arising from the SMA is ligated and divided first. This approach makes it possible to perform total mesopancreas [18] excision, meaning total excision of the second portion of the pancreatic head nerve plexus (PLphII) (Fig. 20.3) [19, 20]. This approach facilitates reconstruction of the portal vein by end-to-end anastomosis.
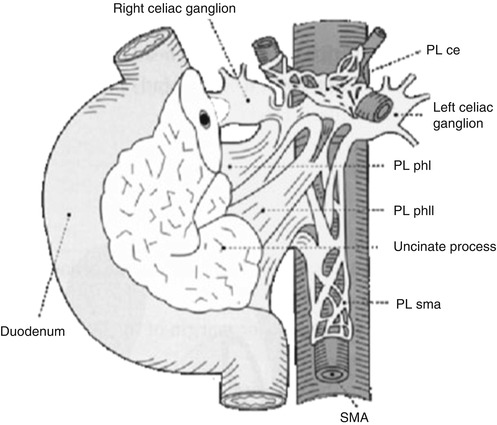
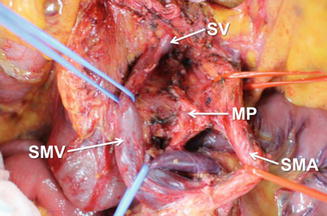
Fig. 20.3
Extrapancreatic nerve plexus (From JPS. Classification of pancreatic carcinoma. 3rd English ed.)
20.2 Surgical Techniques in Isolated PD Using the Nakao Mesenteric Approach
20.2.1 Mesenteric Incision
After laparotomy by upper midline skin incision, the abdominal cavity is examined using ultrasound and washing cytology. The first step in the mesenteric approach is incision of the mesentery from the ligament of Treiz to the lower border of the second portion of the duodenum using electrocautery (Fig. 20.4). The surface of the mesentery is incised until the anterior walls of the SMV and SMA are exposed. With this approach, Kocher’s maneuver is not performed.
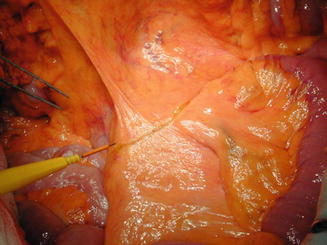
Fig. 20.4
Incision in the mesentery from the ligament of Treiz to the lower border of the second portion of the duodenum
20.2.2 Connective Tissue Clearance Around the SMV and SMA
All of the connective tissues, including the lymph nodes around the SMV and SMA (No. 14d lymph nodes) [17], are dissected to the lower border of the pancreatic head (Fig. 20.5). If no cancer invasion of the second portion of the PLphII is observed, the nerve plexus around the SMA (PLsma) [19, 20] is completely preserved. If cancer invasion into the PLphII or the PLsma is detected, the PLsma is resected to obtain cancer-free surgical margins. If it is difficult or impossible to obtain cancer-free surgical margins, we stop the radical resection. We also stop the radical resection if we determine that reconstruction of the SMV is impossible because of severe cancer invasion into the peripheral branches of the SMV.
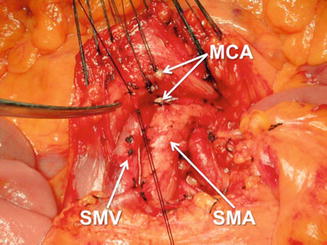
Fig. 20.5
Connective tissue clearance around the superior mesenteric vein (SMV) and superior mesenteric artery (SMA) and division of the middle colic artery (MCA)
20.2.3 Division of the Middle Colic Artery
The middle colic artery is exposed at the anterior side of the SMA. The middle colic artery is generally ligated and divided at the root (Fig. 20.5), which facilitates connective tissue clearance around the root of the SMA (No. 14p lymph nodes).
20.2.4 Division of the Gastrocolic Ligament
The gastrocolic ligament is incised near the transverse colon, and the epiploic sac is opened. By opening the epiploic sac, the mesocolon can be examined from both the anterior and posterior sides, and the anterior surface of the pancreas can be visualized.
20.2.5 Incision of the Mesocolon
The root of the mesocolon is horizontally incised and resected, preserving the arcade of the middle colic artery (Fig. 20.6). This makes it easier and safer to perform connective tissue clearance around the root of the SMA through the large opening in the mesocolon.
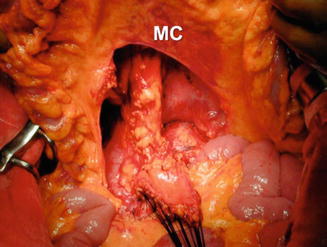
Fig. 20.6
Incision in the mesocolon (MC)
20.2.6 Connective Tissue Clearance Around the Root of the SMA
Connective tissue clearance around the SMV and SMA proceeds to the roots of the SMV and SMA. All connective tissues of the mesenteric root are dissected, including the lymph nodes (No.14 d, p lymph nodes).
20.2.7 Exposing the Mesopancreas
The PLphII is exposed between the uncinate process of the pancreatic head and the SMA (Fig. 20.7). There is no precise anatomical definition for the mesopancreas [18]. In the Japanese classification of pancreatic cancer [19, 20], the anatomy of the extrapancreatic nerve plexuses is described (Fig. 20.3), and Japanese pancreatic surgeons know this anatomy well. I propose that mesopancreas excision means excision of PLphII (Fig. 20.3) and recommend the term PLphII instead of mesopancreas.
 Staging and Determination of Resectability of Pancreatic Cancer
Laparoscopic Distal Pancreatectomy in Pancreatic Cancer
Staging and Determination of Resectability of Pancreatic Cancer
Laparoscopic Distal Pancreatectomy in Pancreatic Cancer
 PET and Other Functional Imaging
PET and Other Functional Imaging
 Mesenteric Approach for Pancreaticoduodenectomy
Mesenteric Approach for Pancreaticoduodenectomy
 Role of Extended Resection in Pancreatic Cancer
Role of Extended Resection in Pancreatic Cancer
 Emerging New Treatment Modalities: Irreversible Electroporation
Emerging New Treatment Modalities: Irreversible Electroporation




Related posts:
Staging and Determination of Resectability of Pancreatic Cancer
Laparoscopic Distal Pancreatectomy in Pancreatic Cancer
PET and Other Functional Imaging
Mesenteric Approach for Pancreaticoduodenectomy
Role of Extended Resection in Pancreatic Cancer
Emerging New Treatment Modalities: Irreversible Electroporation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
