Highlights
- •
Single-port (SP) retroperitoneal robotic partial nephrectomy (RPN) is associated with a significantly longer ischemia time compared to the multiport (MP) approach, despite comparable perioperative and postoperative outcomes.
- •
While the SP platform offers flexibility in accessing challenging tumor locations, its longer ischemia time warrants careful consideration in cases, involving complex renal tumors.
- •
SP RPN is a safe and viable alternative to MP RPN for retroperitoneal tumors.
Abstract
Introduction
Single-port (SP) robotic surgical system performs well in small anatomical spaces, which makes it suitable for retroperitoneal robotic partial nephrectomy (RPN). However, there is limited evidence comparing the safety and feasibility of SP RPN to multiport (MP) RPN. To address this gap in evidence, we sought to analyze and compare the safety of retroperitoneal RPN between SP and MP approaches.
Methods
This is a retrospective cohort study using data from the Single Port Advanced Research Consortium (SPARC) and a multicenter database of patients who underwent retroperitoneal RPN using either SP or MP between 2017 and 2023. Baseline, perioperative, and postoperative data were compared using t- tests, Mann-Whitney U test, χ 2 test, and Fisher exact test. Multivariable analyses were conducted using robust and Poisson regressions.
Results
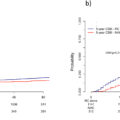
A total of 286 patients (SP RPN, n = 86 [30%]; MP RPN, n = 200 [70%]) underwent retroperitoneal RPN. R.E.N.A.L nephrometry score and tumor location were significantly different between the 2 groups. Notably, the ischemia time was significantly shorter in the MP group (16 vs. SP, 22 minutes, P < 0.001). Adjusting for baseline characteristics, the ischemia time was approximately 7.89 minutes longer for patients in the SP group compared to the MP group, on average (95% CI: 5.87, 9.92; P < 0.001). No significant differences were observed in operative time, EBL, blood transfusion, conversion rates, LOS, PSM, and overall 30-day postoperative complications between the 2 groups.
Conclusion
Our study shows that retroperitoneal SP and MP RPN have comparable perioperative and postoperative outcomes, except for the longer ischemia time in the SP platform. SP RPN is a safe and viable alternative; however, further research is needed to explore its potential benefits, cost-effectiveness, and long-term oncologic outcomes.
1
Introduction
The majority of renal masses are diagnosed incidentally as localized disease, and partial nephrectomy is the recommended treatment for localized renal masses when technically feasible [ , ]. With the increasing application of robotic surgical techniques, the most common approach to nephron-sparing surgery is a robotic partial nephrectomy (RPN) using a multiport (MP) robot [ ]. RPN can be performed using the retroperitoneal or transperitoneal anatomical spaces. Transperitoneal RPN is the more popular approach to perform RPN [ ], despite the reported comparable outcomes between the 2 approaches [ , ]. While the kidney resides within the retroperitoneum, retroperitoneal RPN faces less frequent adoption due to the inherent challenges associated with operating in a confined anatomical space. This smaller working area presents increased difficulty for surgeons.
The purpose-built single-port (SP) robotic platform performs well within small anatomical spaces [ , ] and it can potentially alleviate some of the difficulties in retroperitoneal partial nephrectomy. The access can be performed with a small incision, the instruments can work in a small space without clashing, and the need for peritoneal mobilization is less [ ]. Since 2018, several publications have demonstrated the safe applications of SP retroperitoneal RPN [ ]. However, there is scant data available that compares SP and MP retroperitoneal RPN [ ]. Therefore, an evaluation of the performance of SP in comparison to the well-established MP technique is crucial for informing surgical decision-making and optimizing patient care. The few existing studies are limited by small sample sizes and single-center designs, which may not provide a comprehensive assessment of the SP platform’s efficacy. In this multi-institutional study, we aimed to compare the perioperative outcomes of MP and SP retroperitoneal RPN in terms of the safety, feasibility, and potential benefits of the SP platform. The study aims to contribute to the expanding body of literature and provide guidance for future surgical practice.
2
Patients and methods
2.1
Data source
Data from 2 databases were utilized for this study: the Single-Port Advanced Research Consortium (SPARC) and a multicenter kidney database. SPARC is a prospectively maintained multicenter database of patients who underwent robotic surgery using the SP platform. Specifically, for this study, the database utilized was the SPARC database for robotic nephrectomy. The multicenter kidney cancer database is also a prospectively maintained database of patients who are suspicious of having a renal mass, regardless of the approach used for managing the mass, but excludes the SP platform. Both databases are prospectively maintained and electronically stored at the Icahn School of Medicine at Mount Sinai, New York, and capture similar data on patients’ demographic, clinical, and tumor-related characteristics as well as perioperative and postoperative data. Center-specific institutional ethics review board approval and data sharing agreements were obtained before patient identification, data collection, or de-identified data transfer.
To be eligible for study inclusion, a patient would have had RPN using a retroperitoneal approach via an SP or MP surgical platform between 2017 and 2023 (n = 360). While the MP cases were performed between 2017 and 2023, the SP cases were performed between 2019 and 2023. The robotic system used for all MP cases was the Da Vinci Xi, and the SP cases were performed using the Da Vinci SP (Intuitive Surgical, Sunnyvale, California, USA). We included patients from all centers irrespective of the number of SP or MP cases performed by the centers. We excluded patients with bilateral/multiple tumors (n = 6), and patients missing data on R.E.N.A.L nephrometry score (n = 22), baseline estimated glomerular filtration rates (eGFR) (n = 6), tumor location (n = 36), tumor laterality (n = 1), and body mass index (BMI) (n = 3). Two centers performed both MP and SP, while 4 centers performed MP cases only and another 4 performed SP cases only. Overall, the study cohort consists of 286 patients.
2.2
Study variables
Baseline demographic, clinical, and tumor-specific characteristics considered in our analysis include age, sex, BMI, hypertension, diabetes mellitus, Charlson comorbidity index (CCI), baseline eGFR, tumor size, tumor laterality, R.E.N.A.L nephrometry score, tumor location (anterior, posterior and neither) [ ]. eGFR was estimated using CKD-EPI creatinine equations for glomerular filtration rate [ ]. Pathological variables included are pathologic tumor stage and primary histology.
2.3
Outcome variables
Herein, we evaluated perioperative and postoperative outcomes during and after retroperitoneal RPN. The outcomes of interest were operative time, ischemia time, estimated blood loss (EBL), blood transfusion rate, conversion to open, conversion of radical, length of hospital stay (LOS), positive margin rate (PSM), recurrence rate, and 30-day postoperative complication rate (overall and major complication [Clavien ≥3]) [ ].
2.4
Statistical analysis
Categorical variables are reported as frequencies and percentages, while continuous variables are reported as means and standard deviation as well as medians and interquartile ranges depending on the distribution of the variable.
We compared baseline characteristics, perioperative and postoperative data between both platforms using χ² and Fisher exact tests (when a cell count is <5) for categorical variables and student t test (when the distribution is normal) and Mann Whitney U test (when the distribution is normal) for continuous variables. Multivariable analyses were conducted using robust regressions to evaluate the relationship between the ischemia time, operative time, or EBL and the surgical platform controlling for age, sex, BMI, hypertension, diabetes mellitus, CCI, baseline eGFR, tumor size, tumor laterality, R.E.N.A.L nephrometry score, and tumor location. Similarly, Poisson regression was used to evaluate the relationship between LOS and the surgical platform, controlling for all baseline covariates. All analyses were performed using R version 4.2.2. All P values were 2-sided, and statistical significance was determined at a P < .05.
3
Results
3.1
Baseline characteristics
A total of 286 patients underwent retroperitoneal RPN, with 86 (30%) receiving single-port SP RPN and 200 (70%) undergoing MP RPN. The mean age of the patients was 61 years (SD 12), and 63% were males. Baseline demographic, clinical, and tumor-related characteristics are summarized in Table 1 . We were unable to demonstrate any difference between SP and MP RPN groups in terms of age (60 years [SD 12] vs. 60 years [SD 13]; P = 0.4), or the proportion of males in the study (63% vs. 63%; P = 1). Similarly, there was no statistically significant difference in the mean tumor size (2.70cm [SD 1.32] vs. 2.96cm [SD 1.33]; P = 0.12). However, the SP RPN group had a significantly lower median R.E.N.A.L score (5 [IQR: 4, 7] vs. 8 [IQR: 6, 9]; P ≤ 0.001) and lower proportion of posterior tumors [48% vs. 75%; P < 0.001]. No other significant differences in covariate distributions were observed between the SP and MP RPN groups ( Table 1 ).
| Overall | Multiport | Single port | P value | |
|---|---|---|---|---|
| N | 286 | 200 (70) | 86 (30) | |
| Age, year | 61±12 | 62±13 | 60±12 | 0.4 a |
| Sex | 1 b | |||
| Female | 106 (37) | 74 (37) | 32 (37) | |
| Male | 180 (63) | 126 (63) | 54 (63) | |
| BMI, kg/m 2 | 30 ± 6 | 30 ± 7 | 30 ± 6 | 1 a |
| Hypertension | 175 (61) | 124 (62) | 51 (59) | 0.7 b |
| DM | 57 (20) | 45 (23) | 12 (14) | 0.1 b |
| CCI | 3 (2, 4) | 3 (2, 5) | 3 (2, 4) | 0.005 c |
| Baseline eGFR | 83 ± 22 | 84 ± 21 | 80 ± 24 | 0.3 a |
| Tumor size, cm | 2.88 ±1.33 | 2.96 ±1.33 | 2.70 ±1.32 | 0.12 a |
| Right lateral | 158 (55) | 107 (54) | 51 (59) | 0.3 b |
| R.E.N.A.L score | 7 (5, 9) | 8 (6, 9) | 5(4, 7) | <0.001 c |
| Location | <0.001 d | |||
| Anterior | 33(11) | 16 (8) | 17 (20) | |
| Posterior | 191(67) | 150 (75) | 41 (48) | |
| Neither | 62(22) | 34 (17) | 28 (32) |
Related posts:
 A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
A systematic review of family history, race/ethnicity, and genetic risk on prostate cancer detection and outcomes: Considerations in PSA-based screening
 Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
Neoadjuvant chemotherapy before radical cystectomy in patients with organ-confined and non-organ-confined urothelial carcinoma
 Trends in the use of immediate postoperative intravesical chemotherapy following transurethral resection of bladder tumors
Trends in the use of immediate postoperative intravesical chemotherapy following transurethral resection of bladder tumors
 Prevalence and management of castration-resistant prostate cancer of unknown metastatic status in the real-world setting: The AfroDiTA study
Prevalence and management of castration-resistant prostate cancer of unknown metastatic status in the real-world setting: The AfroDiTA study
 Testosterone recovery after androgen deprivation therapy
Testosterone recovery after androgen deprivation therapy
 Testicular cancer malpractice trends
Testicular cancer malpractice trends
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


