Intrinsic skin aging or physiologic changes are structural, clinical, and immunologic. Secondary changes (wrinkling, coarseness, and roughness) are due to extrinsic factors, such as exposure to ultraviolet rays of the sun.
Terbinafine and itraconazole are safe, have high cure rates in onychomycosis, and require only 3 months of treatment.
Early treatment of herpes zoster with oral antiviral agents halts the progression of the disease, decreases incidence of visceral and cutaneous dissemination, promotes healing, reduces the duration and intensity of acute pain, and reduces the duration and frequency of postherpetic neuralgia.
Treatment of squamous and basal cell carcinoma depends on the size of the lesion and extent or numbers of lesions, morphology, location, and patient’s compliance.
Risk factors for melanoma include very fair skin, family history, dysplastic or numerous nevi, blue eyes, blond or red hair, freckling, frequent sunburn, inability to tan, and immunosuppression.
Seborrheic keratoses have a “stuck-on” appearance, are brown black in color, and occur most commonly on the back, chest, and face. Indications for removal are cosmetic.
Melanoma are infiltrative lesions with diverse coloring—ranging from brown, black, gray to red—with irregular margins.
The best treatment for seborrheic dermatitis of the scalp (dandruff) is prevention using regular shampoos containing tar or selenium sulfide.
Allergic contact dermatitis typically presents as a vesicular or bullous eruption in the area of contact with an allergen around the waist, cap or hat line (rubber lining), or the finger, neck, or wrist (ring, necklace, or watch).
Xerosis occurs more commonly with aging because of a reduction in water contact and barrier function and is best managed by avoidance of frequent bathing or showering with hot water and harsh soaps.
Severe fungal infections of the feet, scalp, and nails are best treated with a course of oral antifungal therapy.
Scabies in the nursing home setting may be epidemic and may present as a seborrheic dermatitis-like rash. Diagnosis is made by the finding of mite excreta or eggs on the hair shaft.
Ulceration of the skin of the lower extremities may result from chronic vascular insufficiency of either arterial or venous origin.
This chapter discusses the common dermatologic conditions of aging. Topics discussed include histologic changes with normal aging (intrinsic) and premature aging (external photoaging). There will be a brief discussion of common benign and malignant lesions, common infections, common papulosquamous disease processes, and a miscellaneous category. No amount of text can fully describe the common dermatologic conditions of aging. Therefore, the chapter text is accompanied in most cases by color plates that characterize most of these skin diseases (also see Table 36.1 for differential diagnosis).
INTRINSIC VERSUS EXTRINSIC CHANGES OF AGING
Skin changes with aging can be categorized as either intrinsic (related to physiologic changes secondary to longevity) or extrinsic (environmentally induced changes). Intrinsic changes can be further subdivided into structural changes, clinical manifestations of these changes, and physiologic and immunologic changes.
Structural changes in the epidermis include flattening of the dermoepidermal interface, generalized loss of melanocytes, focal melanocyte clustering, basal cell heterogeneity, and loss of Langerhans cells. Dermal changes include decreased density, increased size and cross-linking of collagen bundles, elastic fiber loss, decreased vascularity, and reduced ground substance. There is also a decrease in the number of sweat glands, thinning and ridging of the nails, a generalized decrease in the number and thickness of terminal hairs, loss of melanocytes from hair bulbs, focal conversion of vellus to terminal hairs, and decreased innervation and generalized atrophy of tissue.
Clinical changes related to these structural changes include an increased frequency of benign and malignant epidermal neoplasms, irregular pigmentation, a propensity to blister formation, development of lentigo senilis, development of superficial skin laxity, decreased insulating capacity and surface markings, a predisposition to tear-type injury, thermoregulatory disturbances, the development of pallor, xerosis, hypothermia and hyperthermia, brittle nails, diffuse hair loss, coarse hair, hair graying, loss of manual dexterity, propensity to injury, and diffuse thinning of the scalp hair leading to baldness.1,2
Owing to a reduction in dermal clearance of chemical agents with normal aging, older patients have a propensity to persistence of contact dermatitis with slower healing. In addition, the topical administration of potentially noxious medications or chemicals to the skin surface may result in the sudden onset of a severe inflammatory dermatitis because the inflammatory response with aging is delayed at onset. The immune response is also depressed with normal aging such that both the percentage of T cells and its absolute number are decreased. This is directly related to the reduced ability to respond to specific antigens. Clinically, this may manifest as a decline in skin hypersensitivity to specific antigens and the ability to determine immune status. Skin testing with specific agents such as tuberculin, mumps, or Candida may result in a false-negative or weaker hypersensitivity reaction.
An increase in B-cell dysfunction also occurs, resulting in a raised incidence of autoantibodies and increased immunoglobulin-A (IgA) and IgG levels. This may manifest itself clinically as false-positive antigen-antibody reactions between foreign antigens (laboratory reagents to detect clinical disease) and autoantibodies including rheumatoid factor and initial testing for syphilis.
Lastly, the quantity of epidermal 7-dehydrocholesterol per unit area decreases linearly with aging and can result in diminished vitamin D production, development of osteomalacia, and clinical fracture.2
PHOTOAGING
Extrinsic aging of the skin refers to the effects of environmental exposure, principally chronic ultraviolet light exposure. The extent of ultraviolet damage over time depends on the depth of penetration of ultraviolet light in the skin as determined by the wavelength. Ultraviolet radiation involving a wavelength of 290 to 320 nm causes most of the acute and chronic exposure. Wavelengths of sunlight involving 320 to 400 nm are also important in causing damage because they have greater depths of penetration. Ultraviolet light causes damage to skin by effecting DNA injury, decreased DNA repair, or both, as well as oxidation, lysosomal damage, and altered collagen structure.
Clinical correlates of this damage include wrinkling, coarseness, and roughness of skin, with mottled pigmentation. The mottled pigmentation is due to the development of solar lentigos, seborrheic keratoses, ephelides or freckles, hypopigmentation, and telangiectasias. Skin malignancies are also more common in photodamaged areas of the skin.
The role of oxidative stress and the use of antioxidants to prevent extrinsic aging have received much attention in the last several years. Although various in vitro and animal studies have shown that low-molecular-weight antioxidants exert protective effects against oxidative stress (particularly vitamins C and E, ascorbate, tocopherol, and lipoic acid [LA]), controlled long-term studies evaluating the efficacy of low-molecular-weight antioxidants in the prevention or treatment of extrinsic aging are lacking.3
TABLE 36.1 DIFFERENTIAL DIAGNOSIS OF COMMON DERMATOSES IN THE ELDERLY
Treatment of photodamage involves prevention of cumulated exposure through the use of broad-spectrum sunscreens that shield the skin from the effects of ultraviolet light. Tretinoin has been used in high concentrations to reverse some of the cosmetic changes of aging. Tretinoin increases the thickness of the superficial skin layers, reduces pigmentary changes and roughness, and increases collagen synthesis, but only when used for long periods of time. Concentrations of between 0.02% and 0.05% cream have been shown to be an effective treatment option. A recent study demonstrated the effectiveness of a 0.25% solution. This concentration proved tolerable and achieved clinical response in as little as 1 month4 (Evidence Level B). Another study showed that 0.1% cream is superior to 0.05% emollient cream with respect to speed of improvement over a 24-month period5 (Evidence Level B).
α-LA is a potent scavenger with anti-inflammatory properties. It has been shown to be effective in significantly reducing skin roughness when used in a 5% cream and combined with laser profilometry over a 12-week period6 (Evidence Level B). Pyruvic acid, an α-keto acid, when applied in a 50% preparation to achieve a peel, was shown to produce a smoother texture, less-evident fine wrinkles, lightening of hyperpigmentations (freckles and lentigines), thinning of the epidermis, and thickening of the dermis, with limited or no discomfort in the postpeel period7 (Evidence Level B).
Surgical options for the treatment of photodamage include the use of chemical peeling agents, dermabrasion, and laser resurfacing. All of these procedures essentially work by destroying the surface populations of keratinocytes, followed by repopulation of the surface with keratinocytes deep from within the sun-protected follicular structures. Few clinical trials, however, have proved their effectiveness8 (Evidence Level C). One-pass short-pulse erbium: YAG laser has also been shown to be safe and effective, with minimal side effects and rapid healing within 3 to 5 days9 (Evidence Level B). Lastly, the use of 40% urea cream combined with δ-aminolevulinic acid (δ-ALA) with exposure to activating light (photodynamic therapy [PDT]) for 7 days has been compared with the use of δ-ALA and light therapy alone and followed up for 1 and 5 months respectively. Both treatments were found to be safe and effective in significantly reducing the severity of photodamage10 (Evidence Level B).
Although wrinkling may be a sign of photodamage and extrinsic aging, wrinkling in a site with limited sun exposure may be a marker of general health status or intrinsic aging, particularly in women11 (Evidence Level C).
The use of botulinum toxin for treatment of wrinkles has increased greatly in recent years. It is generally used in the following locations: Glabella, brow, crow’s feet, upper lip wrinkling lines, depressor anguli oris, nasolabial folds, mentalis, and neck. Although the treatment is considered to be safe and well tolerated, the injecting surgeon should be familiar with the potential complications of therapy12 (Evidence Level C). Hormone replacement therapy may also slow the progress of intrinsic aging of the skin. However, it does not limit the number and depth of wrinkles13,14 (Evidence Level B).
BENIGN LESIONS
Solar lentigines are circumscribed, pigmented, nonmalignant macular lesions referred to as brown or liver spots. They typically have a diameter of approximately 0.5 cm and are induced by ultraviolet radiation. In rare cases, they may progress into a lentigo maligna melanoma with characteristic diameters in the 3 to 6 cm range and with irregular pigmentation and shape with irregular borders. A change in size or color of the lesion should prompt investigation and resection. Without adequate resection, solar lentigines have a 50% risk of developing into a malignant melanoma and a 10% risk of metastatic spread15 (Evidence Level C).
Sebaceous hyperplasia is a sebaceous gland that has the appearance of a yellow nodule with a central pore. Although the number of sebaceous glands remains stable with age, their size may increase, and sebum production decreases. This results in increased visibility, especially in sun-exposed areas. These lesions should be differentiated from nodular basal cell cancer. Cancerous lesions are differentiated from hyperplasia by the presence of telangiectatic blood vessels and a translucent appearance. Suspicion of malignancy should be followed by biopsy15 (see Fig. 36.1) (Evidence Level C). Treatment options include laser therapy, electrodesiccation, and topical bichloracetic acid. Curettage is a less optimal form of therapy because of scarring. For diffuse multiple lesions, oral isotretinoin has been shown to be effective16 (Evidence Level B).
Milia are epidermal cysts that frequently occur on sun-damaged facial or periorbital skin and measure approximately 1 mm in diameter. Although they may be of concern to the patient for cosmetic reasons, they have no malignant potential. They may be removed with a comedone or needle extractor15 (Evidence Level C).
Acrochordons are skin tags with a flesh-colored appearance and typically occur on the neck and axillae, especially in the obese elderly. They are benign. Indications for removal include cosmetic problems or irritation15 (Evidence Level C). Treatment options include electrocautery or scissor excision at the base of the stalk or cryotherapy. Local anesthesia is usually not necessary.16
Seborrheic keratoses are common in the elderly and typically have a “stuck-on” appearance, are brown black in color, and may occur on any part of the body, but more frequently in seborrheic areas such as the back, chest, and face. The lesions typically range in size from 2 to 10 mm in diameter. Melanomas tend to have more diverse colors ranging from brown, blue, black, and gray to red. In addition, the surface of keratoses is rough as opposed to melanomas in which the surface is smooth. Dermatosis papulosa nigra is a variant that occurs more commonly on the face of dark-skinned individuals, and in multiple ways. Patients have a hereditary predisposition for development and there is no relationship between its occurrence and exposure to sunlight15 (see Fig. 36.2) (Evidence Level C). Excisional biopsy may be required if the diagnosis is in question. Otherwise, because of their cosmetically unappealing appearance, especially with multiple ones, patients will often request removal. Cryosurgery, curettage, and excision are the most common methods of treatment. Except for extremely thick lesions, cryotherapy with liquid nitrogen is effective, but repeat treatments may be necessary. Shaving the lesion or use of curettage with electrocautery after administration of local anesthesia provides an additional option. Although these lesions are typically asymptomatic, keratoses may become irritated or inflamed by chafing with clothing. Topical steroids may be useful for symptomatic relief16 (Evidence Level B).
Senile purpura or ecchymosis involves the development of purplish discolorations in the dermis. They are a result of increased fragility and rupture of the dermal capillaries and blood vessels, with resultant extravasation of blood into the surrounding tissue. Senile purpura is commonly seen on the dorsal forearm and hands. Prevention includes wearing long-sleeved shirts to reduce shear and friction. Caregivers should be cautioned to handle frail patients gently to prevent bruising and skin tears. Patients may need reassurance that the development of senile purpura is not a sign of a bleeding disorder.
Cherry hemangiomas are bright red papules that range from 1 to 5 mm in diameter, increase with advancing age, and appear commonly on the trunk. Although their etiology and pathogenesis are unknown, there appears to be no association with exposure to the sun. Treatment has traditionally involved hyfrecation15 (Evidence Level C). The use of potassium titanyl phosphate (KTP) vascular laser has been shown to be superior to hyfrecation because only one treatment, rather than two, is necessary. There were also fewer side effects with laser therapy17 (Evidence Level B).
Venous lakes, also referred to as benign venous angiomas, are flat, compressible, and soft and range from 4 to 6 mm in diameter. They appear as bluish red lesions most commonly on the lower lips or the ears of older patients. Excision may be indicated for cosmetic reasons or if it cannot be distinguished from melanoma15 (see Fig. 36.3) (Evidence Level C). The use of carbon dioxide vaporization is also associated with excellent cosmetic results that can be achieved in one session18 (Evidence Level B). Infrared coagulation is another option but requires several treatment sessions and is associated with minimal scarring.19
Figure 36.3 Appearance of the lesions of venous lakes, or benign venous angiomas, in the ear. (See color insert.)
Keratoacanthoma is a rapidly growing lesion that typically occurs on the sun-exposed areas of the face and upper extremities with aging. Although usually a solitary lesion, it may present in multiple ways. It may also occur less commonly on the lower extremities in older women. The lesion begins as a papular one, enlarging over a 4-week period to 2 cm or more. An umbilicated, keratinous core develops, and after 4 to 6 months the core is expelled with involution of the lesion, resulting in a hypopigmented scar. Although the exact cause is unknown, ultraviolet light, human papillomavirus, and prolonged exposure to coal tar derivatives are thought to be the risk factors. It is not known whether the lesion is truly benign or has potential for malignancy. However, because of its histologic similarity to squamous cell carcinoma, and potential for scarring, total removal is the preferred treatment for solitary lesions. Small lesions can be treated with electrodesiccation and curettage or through blunt dissection. For lesions occurring around the nose or ears, Mohs surgery (described in detail later in this chapter) provides an alternative. Other alternatives include intralesional fluorouracil, intralesional methotrexate, intralesional 5-interferon-α-2a, or radiotherapy for patients with recurrent or larger lesions16 (Evidence Level B).
DERMATITIS
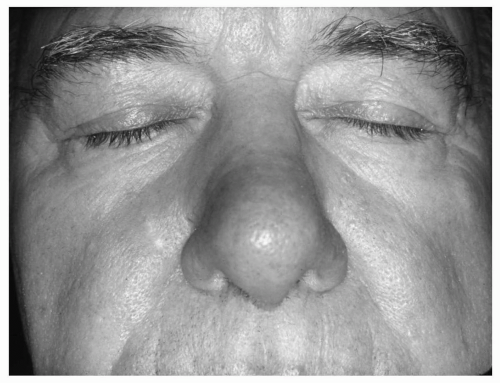
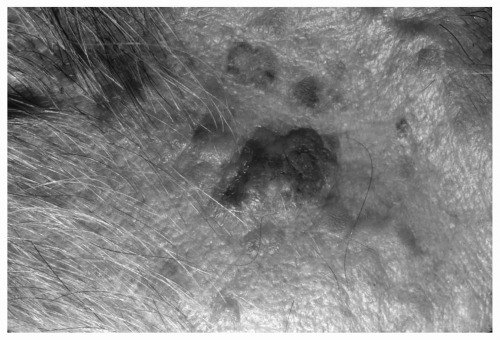
Seborrheic dermatitis principally affects the central part of the face, around the ears and nose, the eyebrows and eyelashes. It can be severe in patients with Parkinson disease and other central nervous system (CNS) disorders, including acquired immunodeficiency syndrome (AIDS). Clinically, it appears as a greasy scaling and erythema of the scalp and skin areas. Pityrosporon orbiculare (Malassezia furfur), saprophytic fungi, have been associated with seborrheic dermatitis but the exact cause is unknown. Treatment of scalp areas involves the use of antiseborrheic shampoos containing tar or selenium sulfide or 2% chloroxine. Treatment of other affected areas includes the use of ketoconazole cream or a mild to moderate potency topical corticosteroid for acute cases. Maintenance therapy, especially for the scalp area, is usually successful in preventing a flare8,15 (see Fig. 36.4) (Evidence Level A). Tacrolimus 0.1% ointment applied for 28 days has been shown to be 70% to 99% effective, with only local burning and irritation as side effects20 (Evidence Level B). Ciclopirox shampoo, which has an active antifungal ingredient, has been shown to be an effective and safe treatment for seborrheic dermatitis of the scalp21 (Evidence Level B). A 4-week treatment of ketoconazole 2% has been shown to be significantly more effective than 1% zinc pyrithione for seborrheic dermatitis of the scalp22 (Evidence Level B). However, lithium gluconate (8%) has been shown to be even more effective than ketoconazole 2% in achieving complete remission at 2 months with comparable safety23 (Evidence Level B).
Figure 36.4 Seborrheic dermatitis—appearing as a greasy scaling and erythema of the scalp and skin areas. (See color insert.)
Allergic contact dermatitis typically presents as vesicles or bullae in the area of contact with an allergen. A clinical cue to the diagnosis is the characteristic location of the lesions around the waist line (belt or rubber lining), cap or hat line, or the finger or neck (ring or necklace). In other instances, a history of recent contact exposure to chemicals or allergens may be helpful in elucidating the cause (e.g., gardening). Mild to moderate symptomatology related to itching and localized distribution may be treated with typical corticosteroids and lubrication, whereas severe symptoms of itching and involvement may require systemic steroids in a dose of 40 to 60 mg per day for 5 to 10 days. With recurrent episodes of dermatitis in which the causative agent is unknown, patch skin testing may be useful15 (see Fig. 36.5) (Evidence Level C).
Xerosis, or dryness of the skin, is common in the elderly and may present simply as rough, itchy skin, or more severely as a scaly, dry, cracked appearance (eczema craquelé). Chronic rubbing and scratching result in thickening or lichenification of the skin. It is the most common cause of itching or pruritus in the elderly. It is due to a reduction in water content and barrier function with aging of the epidermis. Environmental factors such as drying from exposure to hot water, too frequent bathing or showering with harsh soaps, decreased humidity from cold and windy weather (“winter itch”), or dry heat from central heating may exacerbate the process. Common areas of involvement include the anterior legs, extensor aspects of the arms and forearms, and dorsum of the hands. Severe cases can result in cellulitis. Prior to initiating treatment, it is very important to rule out other causes of pruritus such as contact allergens, medications (including vitamins) or foods, metabolic diseases (renal, liver, or thyroid disease), parasitic infections (scabies), anemia, paraproteinemia, papillary duct disease, neoplasia (lymphoma), or psychogenic causes (neurosis). Treatment may require the use of a humidifier, the use of moisturizing agents containing lactic acid or α-hydroxy acids to reduce roughness and scaling, and mild soaps such as Basis or Aveeno. The addition of mild topical steroids may be necessary on an episodic basis when irritation or inflammation is prominent8,15,24 (Evidence Level C). The use of sedating antihistamines such as hydroxyzine and diphenhydramine should be avoided in the elderly because of their anticholinergic properties and risk of precipitating delirium, cognitive dysfunction, functional decline, and other side effects (blurred vision, constipation, urinary retention).25,26 Prevention of exacerbations involves taking tepid and less frequent baths and the regular use of emollients after showering to “seal in” moisture. Older patients should be discouraged from using bath oil because it may make the tub or shower slippery, predisposing the patient to falls8,15 (Evidence Level C). In general, cleansing of the skin with mild synthetic surfactants and/or emollients is ideal for managing xerosis because these agents cause minimal barrier disturbance, allowing the skin to better absorb topically applied agents27 (Evidence Level B). Comprehensive management of xerosis in nursing home residents can prevent stasis dermatitis and ulcer formation, which is discussed in the subsequent text28 (Evidence Level B).
Only gold members can continue reading. Log In or Register to continue