Comanaging Mental Illness in Patients with Diabetes
Comanaging Mental Illness in Patients with Diabetes
Our life is what our thoughts make it.
—Marcus Aurelius, Roman emperor and Stoic philosopher (121-180 AD)
Introduction: The Link between Mind and Body
Unless one’s health is acutely compromised, patients with mental illness coexisting with diabetes should always have the affective disorder stabilized before attempting to improve the metabolic status. Patients who have bipolar depression, schizophrenia, and other forms of affective disorders have a significantly higher rate of suicide. If one is unable to think clearly or make reasonable decisions about one’s personal care, how could one take on the added responsibility of managing a complicated disease such as diabetes? Most patients with diabetes will need to take not only medications for glycemic control but also aspirin, a statin, and multiple antihypertensive agents. Lifestyle interventions such as exercise, dietary modification, home blood glucose monitoring, compliance with appointments, and even picking up prescription refills at the pharmacy in a timely fashion are crucial to successful diabetes management.
Patients with psychiatric disorders have difficulty functioning at work and within their family unit. Productivity and employment are adversely affected by bipolar disorder (BPD) and schizophrenia. Many of these patients are unemployable. More than 60% of patients in the Stanley Center Bipolar Disorder Registry were unemployed, despite the fact that 30% of these individuals had actually successfully completed college.1 The devastating impact of the effects of mental illness in patients with bipolar depression is reflected by the suicide rate, which is 20 times higher than that in the general population and is more likely to occur after repeated episodes of depression.2
Patients with any degree of disabling mental illness will be unable to perform even the basic self-management skills. Therefore, until their emotional status improves and their decompensated mental capacity is stabilized, metabolic control of coexisting diabetes will be virtually impossible. Major depression, schizophrenia, and bipolar depression all increase the risks for diabetes and coronary artery disease (CAD). Because of the undeniable link between emotional unrest and diabetes, patients with mental illness should be screened for coexisting diabetes and vice versa. Treatment for patients with both mental illness and diabetes should focus first and foremost on improving the psychiatric illness with the use of appropriate pharmacologic and behavioral interventions. As one’s cognitive functioning improves, focus may be directed toward treating the metabolic parameters (weight, lipids, blood pressure, glycemic control) to their individualized targets. By comanaging both the mental and physical aspects of the disease state, long-term survivability will be enhanced.
Depression and Diabetes
Although many newly diagnosed patients with T2DM relate the onset of their depression with the time they were initially diagnosed with diabetes, in reality, 80% of patients with diabetes have had a major depressive episode predating their metabolic diagnosis by 6 to 8 years.3 A longitudinal study evaluating more than 11,000 nondiabetic adult depressed patients aged 48 to 67 years determined that those individuals who were most symptomatic had a 63% chance of developing T2DM within 6 years compared with the least symptomatic patients.4
Depression is the most studied psychosocial factor in adolescents with both T1DM and T2DM. The prevalence of depressive symptomatology in this challenging patient population is reported to be between 14% and 33%.5,6 As adolescents with T1DM transition into adulthood, nearly 50% will develop major depression or general anxiety disorder.7 Primary care providers must be trained to screen, and if necessary, initiate appropriate management of younger patients who have coexisting mental illness and diabetes.
Diabetes negatively impacts the health-related quality of life (HRQOL) of patients with T2DM. Interestingly, men with T2DM who experience depression and anxiety have a statistically increased likelihood of mortality versus women who report similar symptoms.8 Instruments that measure HRQOL such as the RAND-36 questionnaire that assesses nine aspects of health status, including physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, mental health, and health change may be useful screening tool in clinical practice. (http://www.rand.org/health/surveys_tools/mos/mos_core_36item_survey.html). The nine categories in RAND-36 may be subdivided into physical (PCS) and mental (MCS) component summaries. Low PCS scores are suggestive of substantial limitations in self-care, physical and social activities, severe body pain, or frequent fatigue. Low MCS scores suggest psychological distress as well as substantial social and role limitations due to emotional dysfunction.9
Patients with diabetes frequently have coexisting affective disorders that may directly affect self-management skills, cardiovascular risk factors, metabolic abnormalities, morbidity, and mortality. Fifteen percent of patients with T2DM meet the diagnostic criteria for an affective illness (depression and anxiety).10 Twice as many women as men have affective disorders.6,11 Major depression disorder (MDD) has been found to be a chronic or recurrent illness in most patients with T2DM. Over a 5-year period, 80% of patients with MDD and T2DM have at least one episode of relapsing depression.12 Compared with patients with diabetes alone, those with depression and diabetes demonstrate poorer self-management skills (following diet and exercise regimens, performing home blood glucose monitoring) and more often fail to refill their prescribed medications.13 Smoking, obesity, sedentary lifestyle, and higher A1C levels are also more common in depressed patients with diabetes.14
Depressed patients frequently adopt a lifestyle that promotes cardiovascular disease. For example, patients with depression tend to be overweight, are physically inactive, and abuse nicotine more than do age-matched controls.3,15 Depressed patients who are overweight [body mass index (BMI) greater than 30 kg per m2] may have poorer long-term outcomes related to diabetes, as these individuals tend to be more resistant to entering weight-loss programs or beginning an exercise regimen.16
Cigarette smoking increases insulin resistance and is a risk factor for progression of many of the microvascular and macrovascular complications of diabetes. Smokers with a history of depression are likely to become even more symptomatic when they attempt smoking cessation, unless they are initially screened and treated for depression.17
Inflammatory mediators also influence the association between depression and diabetes. Patients with major depressive disorders have elevated levels of interleukin (IL)-6 and C-reactive protein (CRP), inflammatory cytokines that are known to cause endothelial cell dysfunction.18 Experimental infusion of another inflammatory cytokine, tumor necrosis factor-α, induced depressive symptoms in human subjects.19,20
Obesity, a precursor to diabetes, is marked by reduced levels of adiponectin. As adiponectin levels decrease, insulin resistance increases, predisposing genetically susceptible individuals to β-cell failure. Inflammatory cytokines released by the liver can reduce the expression of adiponectin.21,22 The elevation in inflammatory cytokines may have a direct influence on future cardiac risk in depressed patients. A study that measured levels of CRP 2 months after depressed patients were discharged from an acute coronary care unit noted that those individuals receiving statins had lower levels of CRP than did patients who were not taking a statin.23
Patients who have major depression have difficulty achieving an A1C level of less than 8%, resulting in a higher incidence of morbidity and mortality, with more frequent and costly hospitalizations. Elevated A1C levels are associated with depression in younger patients. With the exception of elderly patients, improving depression across all age groups has been associated with a significant reduction in glycemic control.24
Although men may experience major depression less often than women, major complications related to diabetes are more often seen in men with coexisting depression and diabetes. As glycemic control deteriorates and complications begin to develop, women appear to be able to bring a more flexible range of coping strategies to the surface, whereas men are more likely to become more passive and accepting of their ultimate fate.25 As patients age and develop more diabetes-related complications, their likelihood of developing depressive symptoms tends to increase as they become more disabled by their disease and face the realization that reversal of their symptoms is unlikely. Older patients become depressed as diabetes begins to have an impact on their quality of life. Difficulty with balance, neuropathic pain, vision problems, sexual dysfunction, and syncope, along with an increasing dependence on additional therapeutic modalities, ultimately cause many patients to realize that their symptoms are irreversible and unmanageable while becoming increasingly more expensive. MDD (major depressive disorder) has been shown to be associated with a 2.3-fold increased risk in mortality for patients with T2DM.26 Patients with coexisting depression and diabetes have more ambulatory care visits, higher pharmacy costs, and incur lifetime medical expenses that are 4.5 times higher than those of individuals with diabetes who are not clinically depressed.27
The biologic mediators that appear to link depression with long-term diabetes-related complications are shown in Table 9-1.
To be successfully treated, the disorders of the mind and the body must both be addressed. Failure to recognize the link between mental illness and diabetes can lead to a higher incidence of diabetes-related complications, especially CAD. Patients with severe mental illness may also be at risk for successful completion of a suicide attempt. Because coexisting diabetes and mental illness is so common, one should consider screening patients with mental illness for diabetes and vice versa. Comanagement with a mental health provider is certainly appropriate for high-risk patients. The use of pharmacotherapeutic agents is warranted in patients with clinical depression. Initially, medications are used to induce remission, whereas the long-term treatment goal should be to reduce the likelihood of symptom recurrence.
• Depression, Diabetes, Microvascular, and Macrovascular Complications: The Metabolic Link
One may question why patients with coexisting depression and diabetes have a higher risk of morbidity and mortality when compared with patients with no clinical evidence of affective disorder. Speculation suggests that depression directly affects the hypothalamic-pituitary-adrenal (HPA) axis.28,29 Some, but not all, depressed patients have elevated levels of corticotrophin-releasing factor (CRF) in their cerebrospinal fluid. This increase in CRF stimulates the HPA to produce high levels of plasma cortisol and induce adrenal hypertrophy. Cortisol, as a counterregulatory hormone, promotes insulin resistance. Patients who have normal pancreatic β-cell function simply produce and secrete more insulin to maintain euglycemia during this enhanced state of insulin resistance. In contrast, patients with prolonged and significant depression, who are obese, physically inactive, and genetically predisposed, will eventually be unable to produce sufficient levels of endogenous insulin to maintain a euglycemic state. As hyperglycemia becomes more severe, pancreatic β-cell function further deteriorates. Patients begin to experience symptoms of chronic hyperglycemia, including polyuria, nocturia, fatigue, visual loss, sexual dysfunction, and neuropathic pain. The physical and emotional stressors associated with major mood disorder and persistent hyperglycemia may lead patients into feeling discouraged about their general state of well-being. They become even more depressed, believing that they are simply prone to developing symptoms associated with the normal aging process for which nothing can be done. Left undiagnosed and untreated, patients’ physical and emotional states of well-being deteriorate rapidly. Fortunately, successful recognition and management of depression can reduce plasma cortisol levels, reverse insulin resistance, and restore the HPA to normal function.29
TABLE 9-1. Mediators of Diabetes Risk, Depression, and Their Possible Link to Long-term Complications
Diabetes Risk Measure
Depression Effect
Effect on Complications
Obesity
Increased weight
Reduced adiponectin
Hypertension
Hyperlipidemia
Proteinuria
Elevated CRP and other inflammatory cytokines
Insulin resistance
Prothrombotic state
Proinflammatory state
Increase in counterregulatory hormones (glucagon, catecholamines, cortisol)
Genes can influence the expression of diabetes-related complications
Adapted from Unger J. Managing mental illness in patients with diabetes. Pract Diabetol. 2006;25:44-53.
Depression also is associated with stimulation of the sympathetic nervous system and higher levels of circulating plasma norepinephrine levels. Resting heart rates are increased, heart-rate variability is enhanced, QT intervals are altered, and baroreflex dysfunction is noted more often in patients with depression when compared with nondepressed controls.30 This suggests that the autonomic derangement in depressed individuals predisposes them to dyslipidemia, insulin resistance, obesity, fatigue, CAD and a higher risk of sudden death.31
Depressed patients have platelet abnormalities that promote a prothrombotic state.32 Drugs that are useful in treating depression, such as serotonin reuptake inhibitors, appear to play a role in limiting this prothrombotic effect.31
Heart disease flourishes within the metabolic milieu of insulin resistance, endothelial cell dysfunction, altered autonomic function, and a proinflammatory state fueled by poor lifestyle and behavioral choices. Excuses abound as to why patients are unable or unwilling to increase their level of physical activity. Nonadherence to treatment protocols is common. As depression worsens and concentration becomes impaired, job performance and family issues deteriorate. Coping mechanisms are lost as life simply becomes too stressful for many patients to manage. Some patients enter into a downward spiral, losing their jobs, health insurance, and depleting their savings accounts. Because diabetes is an expensive disease, patients are quick to discontinue medications that may not directly affect the way that they “feel.” As antihypertensive medications, statins, and even oral hypoglycemic agents are stopped, the metabolic status of the patient rapidly worsens, resulting in irreversible microvascular and macrovascular disease.
• Defining and Screening for Major Depressive Disorder
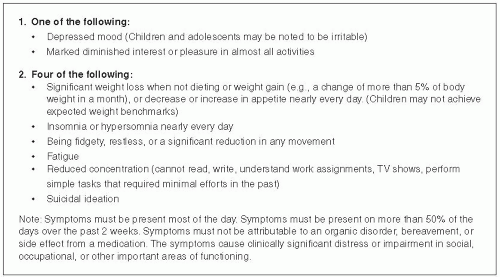
The Diagnostic and Statistical Manual of Mental Disorders (DSM) specifies a set of conditions that must be met to make the diagnosis of MDD.11 Depression is a syndrome consisting of a group of symptoms that occur together, are severe, interfere with normal functioning, and persist daily over a period of at least 2 weeks. One of the symptoms must be depressed mood or anhedonia (absence of pleasure from the performance of acts that would otherwise be pleasurable). The diagnostic criteria for MDD are listed in Figure 9-1. Note that symptoms must be present during the majority of the day, for at least half of the previous 14 days. Bereavement, organic disease, and medication adverse effects must be ruled out as causes of symptoms that may simulate MDD.
MDD is a serious medical disorder that quickly becomes an all-encompassing and incapacitating condition for the patient. Alterations in sleeping and eating patterns result in deterioration in cognitive functioning. Patients are unable to think rationally, much less follow directions on complex treatment protocols. Deterioration of the patient’s mental status often coincides with deterioration of glycemic control and loss of overall metabolic stability. Severely depressed patients are unable to revert to euthymia (a normal functional mood state) without medical intervention. The longer one has unrecognized depression, especially in conjunction with a deterioration in metabolic status, the more likely the patient is to lose the will to live. The potential benefits for recognizing and treating depression in patients with diabetes are listed in Table 9-2.
The early diagnosis and management of depression in our diabetic population can reduce morbidity, mortality, and medical expenses. Unfortunately, nearly everyone would agree that time restraints and reimbursement issues limit one’s ability to practice behavioral intervention in the office setting. PCPs should use effective yet proven means to diagnosis MDD, before embarking on a successful intervention program.
Figure 9-1 • Diagnostic Criteria for Major Depressive Disorder.
(APA. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC: American Psychiatric Association; 1994.)
TABLE 9-2. Potential Benefits of Screening for, Diagnosing, and Treating Depression in Patients with Diabetes in the Primary Care Setting
Improved adherence with prescribed treatment regimen
Improved glycemic control with lowered A1C toward targeted levels
More acceptance by the patient of medically managing coexisting hypertension and hyperlipidemia with behavioral and pharmacologic intervention
Improved compliance related to scheduled office visits with PCP, specialists, and educators
Reduction in anxiety
Restoration of normal sleep patterns
Reduction in severity of chronic pain related to diabetic peripheral neuropathy
Willingness by patient to participate in healthy lifestyle choices such as exercise, smoking cessation, and dietary intervention
Enhanced sexual functioning
Increased likelihood that patient may be willing to participate in community events sponsored by the American Diabetes Association
Increased likelihood that patient will become a more active participant in his or her own diabetes self-management
Increased likelihood that patient will be willing to perform self-blood glucose monitoring
Increased likelihood that patient would be willing to increase the level of intensity of his or her diabetes management, even switching from oral agents to injectable drugs
Promote healthy lifestyle choices and prolong life
PCP, primary care physician.
Adapted from Unger J. Managing mental illness in patients with diabetes. Pract Diabetol. 2006;25:44-53. Copyright by R.A. Rapaport Publishing, Inc.
Although not all patients with diabetes are depressed, many initially demonstrate clues that are strongly associated with coexisting MDD. Patients with a history of depression, anxiety, or substance abuse or a family history of mental illness should undergo periodic screening for MDD. Patients experiencing frequent unexplained hypoglycemia or those who choose to focus on somatic complaints rather than on concerns related to glycemic control should also undergo screening. Patients with diabetic peripheral neuropathic pain often develop sleep disturbances, sexual dysfunction, anxiety disoders, and difficulty maintaining their balance. In time, their neuropathic dysfunction becomes all encompassing, driving their depressive and somatic complaints.
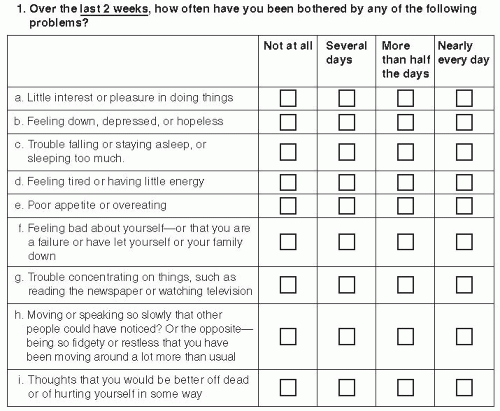
A screening test for depression that has been used effectively for years in the primary care setting is the PRIME-MD (Fig. 9-2). This questionnaire can be completed by the patient with or without assistance from the medical assistant before being seen by the physician. If five of the eight questions are noted to be positive for more than 50% of the days over the previous 2-week period, the patient can be diagnosed as having depression. Further direct questions can then inquire about (a) a history of depression; (b) the age at onset of the first episode of significant depression; (c) a history of suicide ideation or attempt; (d) a family history of mental illness such as depression, bipolar depression, or schizophrenia; (e) what, if any, medications have been used in the past to treat the patient’s depression and for how long the patient was treated; and (f) a history of alcohol or substance abuse. Patients with a positive PRIME-MD should be considered strong candidates for behavioral and/or pharmacologic intervention for depression. Treatment should last for at least 1 year, and possibly longer if (a) the patient had a history of depression, (b) the first episode of depression occurred during the teenage years, (c) the patient had a previous suicide attempt, and (d) the patient has a family history of suicide or depression.
Figure 9-2 • Screening for Depression in Primary Care by Using the PRIME-MD. The PRIME-MD can be used to screen patients for depression. The screening tool has a high sensitivity (73%) and specificity (98%) for the diagnosis of major depression. The criteria for major depression require the patient to have at least 2 weeks of five or more depressive symptoms present for more than half of the days. Note: Developed by Drs. Robert Spitzer and colleagues with an educational grant from Pfizer, Inc. (ris8@columbia.edu). PRIME-MD is a trademark of Pfizer, Inc. (Used from Spitzer R, Kroenke K, Williams J. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study: Primary Care Evaluation of Mental Disorders: Patient Health Questionnaire. JAMA. 1999;282:1737-1744, with permission.)
In patients aged 13 and older who are clinically depressed, the Beck Depression Inventory (BDI)33 may be used to assess the severity of the symptoms. The BDI is a self-administered, 21-item, 4-point rating scale that evaluates mood, pessimism, sense of failure, self-dissatisfaction, guilt, punishment, self-dislike, self-accusation, suicidal ideas, crying, irritability, social withdrawal, indecisiveness, body-image change, work difficulty, insomnia, fatigability, loss of appetite, weight loss, somatic preoccupation, and loss of libido. The BDI is interpreted as follows:
0 to 9, Minimal depression
10 to 16, Mild depression
17 to 29, Moderate depression
30 to 63, Severe depression
The BDI can be downloaded at http://www.psych.upenn.edu/courses/psych001_601_Fall2002/bdi.doc.
Management of Depression in Patients with Diabetes
Once depression has been diagnosed in a patient with diabetes, the importance of medical intervention should be emphasized (Table 9-2). Most patients will be reassured knowing that a physiologic relationship between diabetes and depression is well known, and that depression most often precedes the onset of diabetes by a number of years. Depression is not a permanently curable disease; therefore, goals of therapy must be directed initially at inducing remission and, over the long term, reducing the likelihood of recurrence. Partial remissions tend to increase the chance of recurrence, implying that patients should be treated until they are free of depression symptoms and maintained at this level for a minimum of 1 year.3
Depression should not be viewed as a consequence of diabetes. Simply attempting to improve glycemic control in an attempt to resolve the depressive state is most often unsuccessful.3 The behavioral approaches that may be helpful and self-motivating for depressed patients with diabetes include the following:
Begin a regularly scheduled exercise program. Try an “exercise date night” with their significant other, complete with a personal trainer for motivation. Patients should exercise for at least 30 to 45 minutes each day.
Join the American Diabetes Association (ADA) and attend community events targeting patients with diabetes. Become a community activist for diabetes.
Keep family and friends involved with their daily diabetes care. Allow them to assist in any way possible. Perhaps they can help bring the patient to appointments, remind them to take medications, help prepare meals, rub their feet, assist with self blood glucose monitoring, help administer injections, and join in exercise routines.
The physician should encourage patients to develop a positive attitude toward diabetes self-management. Discouraged patients should be reminded that they are attempting to “think like a pancreas,” a process that is rarely forthcoming, often discouraging, yet absolutely necessary to master to the best of one’s ability. Treating oneself to failure is not an option.
Medical personnel should always find at least one positive attribute that warrants praise during each patient visit. One should never scold a patient, especially those who are making an effort in diabetes self-management programs. Praising patients will offer them hope and encouragement. Labeling patients as “noncompliant” implies that we have failed in our role of medical educators and health-care providers. A patient who consistently fails to show improvement in treatment parameters will often become depressed and discouraged. Such a patient should be helped to think “outside the box” to find other treatment modalities that could be more effective. Ask a colleague or a thought leader in your community for help with the difficult-to-manage patients.
Partnering with a certified diabetic educator (CDE) is certainly warranted for many patients with diabetes. Some patients may have cognitive deficiencies that require “special education skills,” which CDEs are trained to develop. The more patients learn about their diabetes or depression, the more likely they may be to follow the treatment recommendations.
Push patients to break out of their depressive patterns of life. Find something to do that is positive. They can join a club at their church or synagogue, volunteer for a charity or at a local school, or even take a class at a local senior center. Remind patients that they are ultimately responsible for their own happiness in life and that the doctor does not always have a “pill” for everything that ails them. Ultimately, successful management of major depression will depend upon the partnership between the physician and the patient in finding a common ground toward successful interventional strategies.
Don’t do diabetes alone. Many educational opportunities are available for anyone with diabetes. The ADA has an excellent Web site that can assist patients in getting started on their successful self-management program (http://www.diabetes.org).
The physician should place patients on the medical regimen that will most likely result in treatment success rather than promote failure. For example, a patient with T1DM who is having difficulty with glycemic control while taking four daily injections of insulin may do much better on an insulin pump. Once patients perceive that their day-to-day diabetes management is improving, they will be more willing to continue as active participants in diabetes self-care.
Always intensify therapy for patients who are symptomatic. Patients will not feel energetic with an A1C of 11%, especially if they are urinating six times a night, are unable to see clearly, and have lost the ability to obtain or maintain an erection. Continuing patients on oral therapy is bound to worsen their symptoms and their depression. These individuals should be placed on insulin therapy, either by inhalation or by injection.
Depression can occur in anyone whether or not they have coexisting diabetes. However, patients with diabetes may also experience sleep disorders, chronic pain, disordered eating, sexual dysfunction, and even mood disorders as an adverse effect of medications used to treat hypertension, pain, or glaucoma. Low testosterone levels may also contribute to major depression as can illicit drugs and alcohol. Therefore, patients and physicians must have open communication as to the way they are feeling both physically and emotionally so that any depressive symptoms may be aggressively identified and managed.
Always educate patients and their families regarding the link between the mind and the body, depression, and chronic illness. For example, chronic kidney disease results in elevated plasma levels of nitric oxide (NO). High levels of NO can cause sexual dysfunction, weight loss, psychomotor retardation, indecisiveness, and irritability.34 Patients, family members, and coworkers should understand that some behaviors and actions have physiologic etiologies. This explains why most patients with a chronic illness cannot simply “snap out of it” of their own volition without professional guidance. Always remember that major depression is a neurochemically mediated disease state. Once normal neurotransmission is reestablished, major depression and other forms of mental illness should improve.
Good sleep and daily exercise are the least expensive yet most cost-effective forms of antidepressant therapy. Patients should get at least 7 hours of uninterrupted sleep each night. Fragmented sleep, insomnia, sleep apnea, shift work, and circadian rhythm (advanced phase and delayed sleep phase disorders) can adversely affect the neuroendocrine sleep axis, which will increase insulin resistance and cause weight gain. (See chapter on associated sleep disorders.)
Remind patients that although diabetes is a chronic progressive disease, the good news is that most individuals will live their entire life without experiencing any major disrupting event secondary to the disorder. The incidence of eye and kidney disease in the United States is rapidly declining. The likelihood of anyone requiring a limb amputation is very low. The treatment of diabetes today is much more advanced compared to 10 years ago.
Some patients may benefit from cognitive behavioral therapy (CBT), in which they are instructed by psychologists to recognize and remove patterns of negative thought processes that perpetuate depression (e.g., “I am terrible, my life is miserable, and I have no future.”). CBT has been shown to be effective in achieving remission in 85% of patients with T2DM over a 10-week course, and 70% of these patients remained free of depression at the 6-month follow-up visit.35,36
Another example of where CBT may be effective is when patients realize they have a doctor’s appointment in a week, but “all of the blood glucose values are terrible.” They believe that there is “nothing that the doctor can do for me and I will most certainly go blind or lose an eye.” In reality, CBT teaches patients that this is unlikely to happen with today’s array of medical therapies. Most diabetes-related complications may be prevented, delayed, or even reversed if treated intensively. Formation of an optimistic partnership between the PCP, behavioralist, CDE, and family members is an integral aspect of cognitive behavioral therapy. “Doing diabetes alone” is not wise for anyone, whether or not they have any type of mental illness.
CBT shifts the focus away from what patients are doing “wrong each day” to how they are actually being successful with their diabetes self-management. An example of successful CBT was a 71-year-old retired family physician with a 51-year history of T1DM. The patient feared having ANY blood glucose values greater than 160 mg per dL. While using an insulin pump, the patient would monitor his blood glucose levels 8 to 10 times each day. Any blood glucose level greater than 160 mg per dL would be managed with a correction bolus to “get the blood sugar below 100 mg per dL.” The physician experienced episodes of severe hypoglycemia at least three times weekly over the past 6 months necessitating the administration of glucagon by his wife. Despite proudly boasting an A1C of 6.1%, the patient had developed cognitive impairment, which interfered with the safe operation of his insulin pump. Figure 9-3
Only gold members can continue reading. Log In or Register to continue