Comanaging Disorders Commonly Associated with Diabetes
Comanaging Disorders Commonly Associated with Diabetes
Expecting the world to treat you fairly because you are a good person is a little like expecting the bull not to attack you because you are a vegetarian.
— Dennis Wholey, 20th/21st-century self-help author and journalist
Diabetes is associated with a number of chronic disease states often seen within the primary care setting, such as peripheral arterial disease (PAD), pulmonary disorders, Parkinson disease (PD), cancer, sleep disorders, and hearing loss. The pathogenic pathways shared between diabetes and these associated disorders often involve expression of oxidative stress, inflammation, and increased insulin resistance. Recognition of the cause-and-effect relationship may afford primary care physicians a window of opportunity to screen high-risk patients for these important disorders. Conversely, if these ailments are undiagnosed or managed inappropriately, they may adversely affect glycemic control.
Patients with PAD are at risk for critical leg ischemia and amputation as well as coronary artery disease.
Chronic hyperglycemia and hyperlipidemia can induce inflammation of the blood-brain barrier leading to PD in susceptible individuals.
Patients with asthma and chronic obstructive pulmonary disease (COPD) are twice as likely to develop diabetes than age-matched controls. The true challenge for PCPs is to train those patients requiring glucocorticoids how to skillfully manage their gycemic variability.
Patients with diabetes have a higher incidence of all forms of cancer and significantly greater rates of all-cause mortality once diagnosed with a malignancy. Coordination of care between the PCP, oncologist, and other specialists is therefore of utmost importance for these patients.
The neuroendocrine axis of sleep becomes dysfunctional after just one night of insomnia or sleep deprivation. Chronic sleep disorders can increase insulin resistance, promote weight gain, and favor progression of normal glucose tolerance to clinical diabetes.
With nearly 60% of all patients at risk for developing hearing loss between ages 50 and 60 years, periodic audiometric screening for diabetes patients may be appropriate.
Practicing clinicians should find the scientific correlates discussed in this chapter to be intriguing and intellectually challenging. Some of the teleologic links between hyperglycemia and other chronic disease states are unknown even among diabetes specialists. Whereas a PCP may screen a newly diagnosed patient with Parkinson disease for diabetes, the specialist would likely begin managing a patient’s PD by referral, years after the diabetes control has begun to deteriorate. Thus, PCPs have an opportunity to screen, prevent and optimize diabetes care in patients with commonly observed associated disorders.
Peripheral Arterial Disease
The prevalence of PAD in the United States is 5 million persons, or 14.5% of the general population greater than 70 years of age.1 However, the prevalence of PAD is approximately threefold greater in patients with diabetes and more often seen in a younger cohort of individuals (greater than age 50) when compared to age-matched controls.2 Contributing risk factors for PAD include duration of diabetes, age of the patient, hyperlipidemia, body mass index (BMI), smoking history, atrial fibrillation, stroke, renal insufficiency, and a history of coronary artery bypass grafting.3
Clinical Presentation and Pathogenesis
PAD manifests as insufficient tissue perfusion caused by areas of atherosclerosis, which may be acutely exacerbated by embolic or thrombotic disease. The Arterial Disease Detection, Awareness, and Treatment in Primary Care (PARTNERS) study screened asymptomatic patients in 350 primary care offices within the United States for PAD. Patients eligible for screening [using ankle brachial index (ABI) testing] included those aged ≥70 years, or persons aged 50 to 69 years with a history of cigarette smoking or diabetes. PAD was detected in 29% of the 7,000 patients screened.4 Fewer than 10% of patients with PAD had classic symptoms of exercise-induced claudication. The vast majority of patients experienced “atypical symptoms.” Moreover, only 49% of physicians correlated patient symptomatology as being representative of PAD prior to screening.
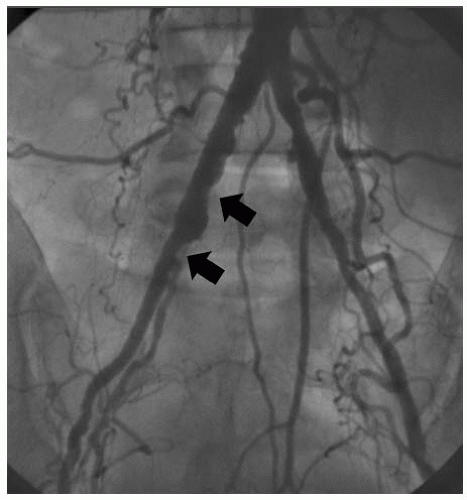
During exercise, blood flow cannot maximally increase through muscles oxygenated via proximally occluded arteries. When the metabolic demands of the muscle exceed blood flow, claudication ensues. Patients also experience a longer recovery period for claudication to ease, during which time normal blood flow resumes within the affected muscle. Aortoiliac disease (Fig. 8-1) manifests as pain in the thighs and buttocks, whereas femoral-popliteal PAD presents as calf pain. Symptoms of PAD are precipitated by walking a predictable distance and are relieved by rest.
PAD is characterized as being either acute or chronic, each with different etiologies (Table 8-1). Acute ischemia most often results from an embolus originating from the heart (secondary to valvular insufficiency or atrial fibrillation). Alternatively, the origin of an embolism can be debris from an atherosclerotic plaque in the aorta or a large peripheral vessel such as the superficial femoral artery. The embolic occlusion most commonly occurs at the arterial bifurcation points of the aorta, iliac, femoral, or popliteal artery. Patients experience a sudden onset of lower extremity pain initially in the feet and toes, which progresses proximally within a short time. The symptoms may be partially and temporarily relieved by placing the extremity in a dependent position. In chronic disease, symptoms are less severe because collateral circulation around the occluded vessel is well developed, minimizing the pain of exercise-induced ischemia.
Patients with chronic PAD will typically relate their onset of pain to a particular walking distance (e.g., 1 block claudication). Claudication due to PAD is reproducible within the same muscle group that has obstructed arterial flow. The pain stops within 2 to 5 minutes of initiating rest. Chronic arterial occlusive disease may be difficult to diagnose prospectively because many patients have atypical claudicatory symptoms. Screening patients at risk for PAD using a Doppler ABI may allow physicians the opportunity to identify patients with PAD and initiate a proactive approach to slow disease progression.5 More importantly, these patients are at higher risk for cardiovascular ischemic events and mortality. Identifying patients with PAD will allow the timely initiation of statins and antiplatelet agents.
Figure 8-1 • A 56-year-old T2DM Patient Who Presents for Heart Catheterization Due to Medical Failure of Antianginal Drugs. Prior to heart catheterization, the patient was noted by the nurse to have poor leg pulses. This patient has significant right-sided aortofemoral disease (arrows) secondary to severe atherosclerosis. (Photograph courtesy of Robert Chilton, DO.)
TABLE 8-1. Differentiation of Acute and Chronic Peripheral Arterial Disease
History of cardiac catheterization, hypertension, diabetes, smoking, family history of CVD, hyperlipidemia
Etiology
Embolic
Occlusive mural thrombus
Historical clues
No prior history of intermittent claudication
History of intermittent claudication
Known source of embolic etiology
History of coronary heart disease
Clinical signs
Limb is pale and pulseless
Paresthesias develop followed by paralysis
May be asymptomatic or symptoms may be atypical
Pain with ambulation; subsides with rest
Hair loss
Brittle nails
Dry, scaly, atrophic skin
Dependent rubor
Pallor with leg elevation after 1 min at 60 degrees (normal color should return in 10-15 sec; longer than 40 sec indicates severe ischemia)
Ischemic tissue ulceration (punched-out, painful, with little bleeding), gangrene
Absent or diminished femoral or pedal pulses
Arterial bruits
Pain trigger
Acute embolic etiology or in situ plaque thrombosis
Intermittent claudication, characterized by cramping, tightness, or tired sensation induced by exercise
Pain location in buttock, hip, thigh, calf, foot
Distance to claudication is consistent
Pain does not occur with standing and is relieved by cessation of activity
Appearance
Fixed, mottled, cyanotic limb
Ischemic, necrotic toes, with multiple erythematous granulating lesions on dorsum of foot (Note, most patients have no visual findings on examination)
Diagnostic workup
Arteriography
ABI for screening
Magnetic resonance angiography for imaging large and small vessels
Treatment
Anticoagulation
Thrombolytic therapy
Surgical intervention
Embolectomy
Percutaneous angioplasty
Improved walking distance and ABI have been attributed to smoking cessation
Walk 45-60 min daily. Walk until claudication occurs. Rest until pain subsides, then resume exercise.
Customize the metabolic management of patient’s disease state. Control diabetes, lipids, and blood pressure
Cilostazol (Pletal) 50-100 mg b.i.d
Percutaneous angioplasty followed by surgical intervention
Stenting
Adapted from Cronenwett JL, Warner KG, Zelenock GB, et al. Intermittent claudication: current results of nonoperative management. Arch Surg. 1984;119(4):430-436; Couch NP. On the arterial consequences of smoking. J Vasc Surg. 1986;3(5):807-812; Conen D, Everett BM, Kurth T, et al. Smoking, smoking status, and risk for symptomatic peripheral artery disease in women: a cohort study. Ann Intern Med. 2011;154(11):719-726; Rowe VL, Lee W, Weaver FA, et al. Patterns of treatment for peripheral arterial disease in the United States: 1996-2005. J Vasc Surg. 2009;49(4):910-917; Krajewski LP, Olin J. Atherosclerosis of the aorta and the lower extremities. In: Young JR, Graor RA, Olin J, Bartholomew JR, eds. Peripheral Vascular Diseases. Chicago, IL: Mosby Year Book; 1991:18.
Screening Patients for PAD
PAD predicts future all-cause mortality. A recently published observational study of 6,292 patients suggested that patients with diabetes and hypertension [but no prior history of cardiovascular disease (CVD)] who had a normal resting ABI had a 41.2% 10-year mortality rate if their postexercise ABI was less than 0.85. Therefore, ABI screening, especially if performed after an exercise session, may be a powerful predictor of all-cause mortality in high-risk patients.6
Why should an abnormal postexercise ABI be predictive of all-cause mortality? At baseline, a healthy person may have a higher measured ankle pressure than arm pressure. When exercise begins, no change in measured blood pressure occurs in the healthy extremity as there is little or no evidence of atherosclerosis that would narrow the vessels. In the atherosclerotic limb, each stenotic segment acts to reduce the pressure head experienced by distal muscle groups. Correspondingly, at rest, the measured blood pressure at the ankle is less than that of a healthy person. Once physical activity starts, there is increased demand for blood flow by the exercised muscles. The narrowed vessels are unable to accommodate the increase in blood flow required, and distal pressure is further reduced.
The phenomenon of increased blood flow causing decreased pressure distally to an area of stenosis is based on Poiseuille’s law (Fig. 8-2). In the 19th century, this French physician performed numerous experiments using liquid and cylindric tubes. He observed that flow rate of liquid through a tube is proportional to the radius of the cylindrical tube raised to the fourth power and inversely proportional to the length of the tube and the liquid viscosity. Thus, the radius of the blood vessels is the most important factor in determining the blood flow rate. If the radius of a peripheral vessel (or coronary artery) is decreased by 50%, the blood flow through that vessel will decrease 16-fold.
In 2011, the American College of Cardiology Foundation and the American Heart Association Task Force published updated guidelines for the management of patients with PAD.7 Patients with diabetes should be screened for PAD based on their recommendations shown in Table 8-2.
Performing the Ankle Brachial Index Test
ABI testing is a simple, painless procedure that may be performed within the primary care office (Fig. 8-3). Initial equipment costs are approximately $2,300 to $6,000. The procedure is reimbursable by private payers and Medicare under CPT Code 93922. ABI pressures must be measured using both the posterior tibial (PT) and the dorsalis pedis (DP) arteries. To calculate the ABI for each leg, simply use the higher of the DP or PT pressures divided by the higher of the brachial pressures from the arms. Prior to billing under CPT code 93922, discuss which ICD-9 codes are covered by each insurer for the procedure. Testing requires less than 10 minutes and may be performed by a medical assistant. The computerized interpretation printout provides a hard copy for the patient’s medical record. If the ABI does not provide a hard copy of the results, the evaluation is considered to be part of the E/M service and is not separately reportable.
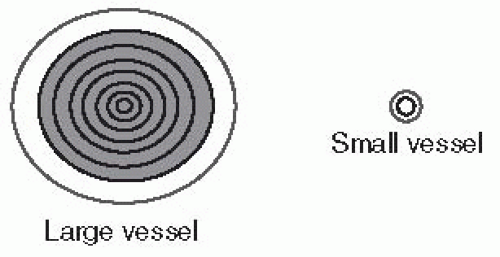
Figure 8-2 • Poiseuille’s Law. The relationship between conductance and diameter can be explained by considering the “layers” of blood in a vessel. Per Poiseuille’s law, the velocity is derived by integrating the velocities of all concentric rings of flowing blood and multiplying them by the areas of the rings. A small vessel has a large proportion of blood in contact with the walls. A larger vessel has fewer layers of blood in contact with the walls. The radius of a given vessel is the most influential factor of blood flow through that artery. Blood flowing through a large artery meets with very little resistance. However, if the radius of the artery is narrowed, resistance is raised to the fourth power and additive when two or more occlusive lesions are located sequentially within the same artery. (Modified from Sutera SP, Skalak R. The history of Poiseuille’s law. Ann Rev Fluid Mech. 1993;25:1-19.)
TABLE 8-2. Recommendations for Performing ABI Screening for Detecting Peripheral Arterial Disease in Patients with Diabetes
• A resting ABI should be used to establish the diagnosis of PAD in high-risk patients. The ABI is calculated as the ratio of systolic blood pressure at the ankle to the arm.
• High-risk patients include those with exertional claudication, nonhealing wounds, age ≥65 y, or those age ≥50 y with a history of smoking or diabetes.
• Normal ABI values are defined as 1.00-1.40.
• Borderline ABI values are defined as 0.91-0.99.
• Abnormal ABI values are defined as ≤ 0.90
Adapted from Rooke TW, Hirsch AT, Misra S, et al. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (Updating the 2005 Guideline). A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:00-00. DOI: 10.1161/CIR.0b013e31822e80c3.
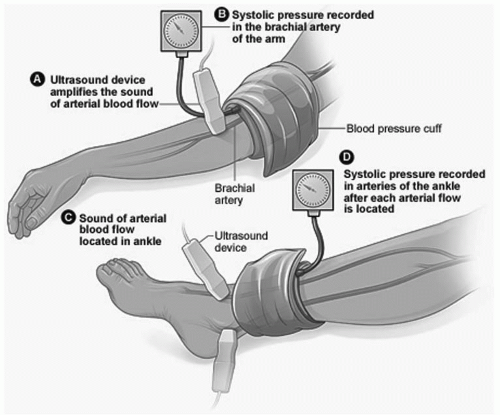
Figure 8-3 • Ankle Brachial Index Examination. A blood pressure cuff is applied to the patient’s arm and inflated. A Doppler ultrasound placed at the radial artery is used to record the first sound as the cuff is deflated. The cuff is then applied to the other arm and the procedure is repeated. The highest of the two arm blood pressures is accepted as the “baseline” upper extremity reading. The cuff is then applied to the midcalf on one leg and inflated. The Doppler ultrasound is placed at the dorsalis pedis (DP) and the posterior tibial (PT) arteries to record the first sound as the cuff is deflated. The cuff is then placed on the opposite leg, and the procedure is repeated. The highest ankle pressure for each leg is used as the lower extremity “baseline” reading. The ratio of each ankle to brachial pressure is determined by dividing the ankle by the highest brachial pressure. An equal ratio implies no blockage of blood flow into the lower extremities. If the ratio of blood flow into the ankles is less than 0.9, PAD is likely to exist. A ratio of less than 0.8 correlates with symptomatic exercise induced claudication. Patients with a ratio of less than 0.4 are likely to experience pain at rest in their legs. Severe, limb-threatening PAD is diagnosed when the ratio is less than 0.25.
ABI measurements may actually be misleading in patients with diabetes because the presence of medial calcinosis renders the arteries incompressible. False elevations in ABI readings will result in suprasystolic ankle pressures (ABI > 1.3). Patients suspected of having a false elevation in their ABI readings should be referred to an accredited vascular lab where measurements of digital arterial systolic pressure (toe pressure), transcutaneous oxygen tension, and/or pulse volume recordings may be performed.8
Management of Patients with PAD
Patients with typical symptoms of intermittent claudication represent fewer than 20% of patients with objective evidence of PAD.9 Patients with lifestyle-interfering claudication and evidence of aortoiliac disease should undergo primary stenting as the initial therapy. Proximal atherosclerotic disease does not respond well to exercise and medical therapy. The long-term patency rates for conservative care approach those of surgical interventions without the associated morbidity, prolonged hospital stays, and recovery time.9
Those with disease below the inguinal ligament should undergo a trial of medical therapy consisting of a walking program and cilostazol (Pletal) 50 to 100 mg b.i.d (assuming no history of heart failure). Cilostazol has been shown to improve walking distance in patients with stable intermittent claudication in eight large randomized placebo-controlled, double-blind trials of 12 to 24 weeks.10 If the patient does not respond to a 4-month trial of conservative management, a revascularization procedure should be considered. Nevertheless, patients with claudication progress to limb loss at a low rate of approximately 5% per year. Therefore, revascularization is best reserved for patients with favorable anatomy who fail conservative therapy and have lifestyle or vocational limiting symptoms. The therapeutic goals for such patients are symptom relief, increased walking distance, and improved functionality and quality of life.
Patients with critical limb ischemia (CLI) (rest pain, nonhealing ulcers, or gangrene) have more extensive disease than patients with intermittent claudication. As such, these individuals require a more urgent revascularization approach for limb salvation. Patients with diabetes and CLI have multilevel disease involving arteries below the knee in addition to small-vessel (microvascular) disease that may not improve even with revascularization. Patients with diabetes who smoke and present with CLI are 10 times more likely to require a nontraumatic lower extremity amputation than agematched controls.9 More than half of all lower extremity amputations occur in patients greater than 80 years of age. The clinical outcome for patients presenting with CLI is grim. Within 3 months of presentation, 12% will require an amputation and 9% will die.9
The 1-year all-cause mortality rate for patients with CLI is 22%. The Bypass versus Angioplasty in Severe Ischaemia of the Leg trial compared an initial strategy of angioplasty with vascular surgery in 452 patients with CLI.11 The primary outcome was time to amputation or death (amputation-free survival) over 6 months. There was no statistical difference between the groups for quality of life outcomes. For the first year of follow-up, costs associated with a surgery-first strategy were higher than for angioplasty. Thus, percutaneous intervention first strategy appears to be the intervention of choice for patients who are candidates for either surgery or percutaneous angioplasty. Aortoiliac and aortofemoral bypass procedures are associated with 74% and 95% 5-year patency rates, respectively, which are comparable, yet not superior to percutaneous therapies.12,13
Patients with aortoiliac disease are being managed with percutaneous kissing-balloon-expandable stents designed to scaffold the lumen and prevent embolization rather than simply employing balloon angioplasty.14
Medical therapy, percutaneous angioplasty, and surgery have been compared in several trials in symptomatic patients with femoral-popliteal disease. While angioplasty may provide for a better short-term improvement in claudication, the benefits of exercise are not only longer lasting but also multifactorial and should always be the initial treatment recommendation in these patients.15 Revascularization procedures (either angioplasty or surgery) offer significant advantages compared with medical therapy for improvement in walking distance.16
Peripheral artery stents may be recommended as salvage therapy for patients with femoral, popliteal, and tibial PAD who have failed angioplasty (residual diameter stenosis greater than 50% or flow-limiting dissection).17 Stents may also be feasible for long or heavily calcified lesions.
Below-knee angioplasty is reserved for patients with CLI or those individuals with severe claudication due to extensive multilevel disease. Limb-salvage rates at 2 to 5 years are 80% to 90% with modern endovascular techniques.9 Success is determined by relief of rest pain, healing rate of ulcers, and avoidance of limb loss.
Newer therapies for the minimally invasive endovascular treatment of claudication and CLI include rotational and orbital atherectomy for which there are no long-term or comparative results. Short-term results have been promising, but these technologies may be more expensive than conventional therapies. At this time, surgery still provides the best long-term patency and limb salvage results when compared to all other modalities. Alternatively, surgical revascularization is associated with higher morbidity and mortality rates than endovascular therapies. Which modality to choose for a particular patient depends upon the pattern and extent of arterial disease, indications for the procedure, coexisting complications, and the projected life span of the patient. Clinical trials are currently assessing the safety and efficacy of minimally invasive drug-eluting stents as well as balloon and biodegradable stents. These devices may provide better long-term patencies and improved limb salvation outcomes while lessening the morbidity associated with surgical revascularization.
A summary of the current recommendations for medical and surgical interventions related to PAD is displayed in Table 8-3.
Parkinson Disease
The risk of PD is approximately 40% greater among patients who have had diabetes for longer than 10 years compared with euglycemic individuals.18 Common pathogenic processes such as chronic inflammation or oxidative stress may first lead to diabetes and then, years later, to a higher risk of PD. Diabetes may also predispose patients to insulin dysregulation and subsequent neurodegeneration. Insulin receptors are expressed in the substantia nigra. The two major neuropathic findings in patients with PD are loss of pigmented dopaminergic neurons in the substantia nigra and the presence of Lewy bodies. Approximately 70% of dopaminergic neurons are lost before the motor signs of PD emerge. Although Lewy bodies are not specific to PD, their presence within the substantia nigra is believed to represent the presymptomatic phase of the disorder.19
Patients with PD demonstrate decreased stimulation of dopamine within the basal ganglia.20 In animal models, reduced dopamine levels are observed in the insulin-resistant state and normalize as rodents become insulin sensitive.21 Consistent with these observations in animals, administration of bromocriptine (a sympatholytic D2-dopamine agonist) improves glycemic control in patients with T2DM.22
Hyperglycemia, which contributes to endothelial dysfunction, may also favor neurodegeneration as supported by the association between PD incidence and diabetes duration.23 Insulin acts as a growth factor in the brain and reduces oxidative stress, whereas insulin resistance decreases the transport of insulin into the brain.24 The densely concentrated insulin receptors located in the substantia nigra appear to play a role in the expression of central dopamine concentrations, which is deficient in PD.25
TABLE 8-3. Management of Patients with Peripheral Arterial Disease
Management Modality
Recommendations
Smoking cessation
Patients who smoke or former smokers should be asked about status of tobacco use at every visit
Counsel patients on smoking cessation at every visit
Unless contraindicated, pharmacologic interventions may include varenicline, bupropion, and nicotine replacement therapy
Antiplatelet therapy
Antiplatelet therapy can be useful to reduce the risk of MI, stroke, or vascular death in asymptomatic individuals with an ABI ≤0.90
Aspirin 75-325 mg/d is recommended as safe and effective therapy to reduce the risk of MI, stroke, or vascular death in patients with symptomatic PAD, CLI, prior lower extremity revascularization, or prior amputation for lower extremity ischemia
Clopidogrel 75 mg/d is an effective alternative antiplatelet therapy to aspirin to reduce the risk of MI, ischemic stroke, or vascular death in patients with symptomatic PAD, CLI, prior lower extremity revascularization, or prior amputation for lower extremity ischemia
The combination of aspirin + clopidogrel may be considered to reduce the risk of CV events in patients with symptomatic atherosclerotic PAD
Warfarin is of no benefit and is potentially harmful when used in patients with PAD due to an increased risk of major bleeding
Critical limb ischemia: Endovascular and open surgical limb salvage
Patients with combined inflow and outflow disease with CLI should have inflow lesions addressed initially
For patients with combined inflow and outflow disease in whom symptoms of CLI or infection persist after inflow revascularization, an outflow revascularization procedure should be performed
Balloon angioplasty is reasonable to perform for patients with limb-threatening lower extremity ischemia and an estimated life expectancy of ≤2 y to improve distal blood flow
For patients with limb-threatening ischemia and an estimated life expectancy of ≥2 y, bypass surgery is reasonable to perform as the initial treatment to improve distal blood flow
Adapted from Rooke TW, Hirsch AT, Misra S, et al. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (Updating the 2005 Guideline). A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:00-00. DOI: 10.1161/CIR.0b013e31822e80c3.
T2DM and hyperlipidemia may induce a chronic inflammatory pathway, leading to destruction of both pancreatic islet β-cells and dopaminergic neurons in the substantia nigra. The brain is considered an immunologically privileged organ, free from immune attack due to the protection afforded by the blood-brain barrier. However, with aging and under conditions of chronic inflammation, the blood-brain barrier becomes breached and more permeable. Consequently, proinflammatory factor, reactive oxygen species, and neurotoxins may cross the blood-brain barrier and induce neurodegeneration. Both central and peripheral inflammation appears to be dysregulated in patients with PD.26
Although the direct relationship between PD and diabetes is unclear, patients with PD should certainly be screened for diabetes and lipid disorders. What is uncertain is whether improving one’s hyperglycemia or other metabolic abnormalities will influence outcomes for patients who are afflicted with both disorders.
Anectodotal observations suggest that some patients with advanced PD and symptoms such as dysphagia and bradykinesia and diabetes may experience temporary improvement with exenatide and exanatide LAR. However, additional clinical trials must be performed prior to advocating the preferential use of any antidiabetes drug in patients with PD.
COPD, Asthma, and Glucocorticoid-induced Hyperglycemia
In a prospective cohort study involving 100,000 women, subjects with COPD had a statistically significant increased risk of developing T2DM.27 Inflammatory markers that are increased in patients with T2DM have been observed to be up-regulated in patients with COPD, suggesting that inflammation may be a common link. Elevated levels of CRP, IL-6, and TNF-α are linked to the development of insulin resistance in T2DM, supporting a role for inflammation in the pathogenesis of diabetes.27 In addition, patients with COPD tend to minimize their exercise capacity, leading to an increase in adipose tissue mass and a subsequent rise in systemic markers of inflammation. The link between systemic inflammation may be persistent even when weight loss is not apparent.28
A population-based retrospective database study comparing medical records of 2,392 patients with asthma with those of 4,784 age-matched controls suggested that the incidence rate for diabetes was 188.6 per 100,000 versus 134 per 100,000 within the control group. Patients with asthma are twice as likely to have coexisting diabetes.29 The hazard ratio for CVD in this study was 1.48 (p = 0.0349) indicating that a diagnosis of asthma increases one’s probability of developing both diabetes and heart disease. The authors of the study suggest that inflammatory, environmental, and genetic mechanisms may be implicated as mediators for all three disease states.
Youths with dual diagnoses of T1DM and asthma have a higher mean A1C than those with diabetes alone (7.77% vs. 7.49%; p = 0.034). Younger patients treated with leukotriene modifiers, either as monotherapy or in combination with rescue or other inhaled medications, had the best glycemic control. A total of 72% of these patients were considered as having “good control” among all groups of medication users. Those patients who were receiving no drug therapy for asthma had the highest A1Cs in the study.30 The suggestion is that specific asthma medications may both decrease systemic inflammation and have a positive effect on long-term glycemic control.
Effect of Glucocorticoids on Glycemic Control
Patients with diabetes and coexisting COPD or asthma may require glucocorticoids during periods of acute exacerbations. Other patients, such as those with rheumatoid arthritis, are often prescribed maintenance doses of steroids. Glucocorticoids are not only the most common cause of drug-induced diabetes, they also are likely to induce severe postprandial hyperglycemia in patients with preexisting diabetes.
Glucocorticoids induce a state of insulin resistance rather than decrease insulin production. In euglycemic subjects, the liver decreases its glucose output in response to insulin. However, glucocorticoids decrease the liver’s sensitivity to insulin, thereby increasing hepatic glucose output.31 Steroids also inhibit glucose uptake in muscle and fat, reducing insulin sensitivity as much as 60% in healthy volunteers due to a postreceptor defect.32 The peak effect of prednisone on glycemic excursions occurs between 4 and 6 hours after dosing and persists for up to 16 hours.
Prednisone does not affect fasting plasma glucose levels if given once daily in the morning at doses of ≤30 mg. Short-term medium-dose prednisone (20 mg per day for 3 days induces postprandial hyperglycemia in T2DM and in patients with prediabetes from midday to midnight due to suppression of insulin secretion followed by decreased insulin action that dissipates overnight.33 Insulin requirements may double, depending on the glucocorticoid dose. For patients with T1DM taking prednisone 60 mg daily for 3 days, mean blood glucose levels increased 30 mg per dL and persisted for 24 hours after the drug was discontinued. Insulin doses increased on average 69% for patients with T1DM using prednisone for just 3 days.34
Targeted Glycemic Management for Patients with Diabetes Using Glucocorticoids
The random or 1 to 2 hour postprandial glycemic target for patients treated with chronic or acute steroid therapy is less than 220 mg per dL. Patients with T2DM should have their doses of OADs titrated to minimize these postprandial excursions as shown in Table 8-4.
Glucose levels exceeding 300 mg per dL result in symptomatic hyperglycemia (e.g., fatigue, polyuria, polydipsia) as well as activation of oxidative stress pathways favoring vascular inflammation. Patients managing asthma or autoimmune disorders with chronic steroids will either need to initiate insulin therapy or adjust their prescribed dose of insulin based on postprandial glycemic excursions.
Patients who had been using only basal insulin and have not experienced a significant increase in fasting glucose levels should minimize postprandial excursions by initiating a rapid-acting analogue (lispro, glulisine, or aspart) at each meal. The dose of the rapid-acting insulin is calculated as 0.1 U per kg per meal. Thus, a 100-kg person would require 10 U of insulin injected 15 minutes prior to eating. Due to the increased insulin resistance caused by the use of prednisone, consider increasing the baseline dose of prandial insulin by 10% to 20% targeting a 2-hour postmeal glucose value of less than 180 mg per dL. Patients who also experience a rise in fasting glucose levels while on steroids can increase their basal insulin dose by 1 U each night until their fasting levels are less than 110 mg per dL.
TABLE 8-4. Therapeutic Options to Optimize Glycemic Control for Patients Using Glucocorticoids
Random or 1-2 Postprandial Glucose 140-220 mg/dL
Random or 1-2 Postprandial Glucose 220-300 mg/dL
Random or 1-2 Postprandial Glucose >300 mg/dL
Suggested Therapeutic Options
Metformin 850-100 mg b.i.d with food
DPP-4 inhibitor
GLP-1 agonist
Meglitinides (longer-acting forms of sulfonylureas may not be suitable if the fasting plasma glucose is normal)
Adapted from Lansang MC. Glucocorticoid-induced diabetes and adrenal suppression: how to detect and manage them. Cleve Clin J Med. 2011;78 (11) 748-756.
Patients who are insulin naive and require chronic glucocorticoid therapy may also be placed on a mixed insulin analogue (bi-aspart 70/30, lispro mix 50/50, and lispro mix 75/25). The initial dose may be calculated as 0.3 U per kg per day. For example, a 100-kg patient with T2DM who has been taking a DPP-4 inhibitor plus metformin should add 30 U of a mixed insulin analogue once daily at lunch if postprandial glucose values consistently exceed 300 mg per dL. Dose titrations should be made every 2 to 3 days until the patient has achieved the 2-hour postmeal glucose target of less than 180 mg per dL.
Frequent paired glucose testing should be suggested for all diabetes patients using acute or chronic steroid regimens. Glucose values are monitored fasting, as well as before and 2 hours after each meal. Normal 2-hour postprandial excursions should not exceed 50 mg per dL from baseline. For example, if the prelunch glucose level is 125 mg per dL, the 2-hour postprandial glucose value should be less than 175 mg per dL. Patterns suggestive of extreme postprandial or fasting glycemic excursions would require adjustments in insulin dosing.
While tapering off steroids, glucose levels will also need to be assessed. Within 24 hours of reducing the prednisone dose to less than 7.5 mg per day, patients may be at risk of developing iatrogenic hypoglycemia unless insulin dosing is downtitrated.
Cancer
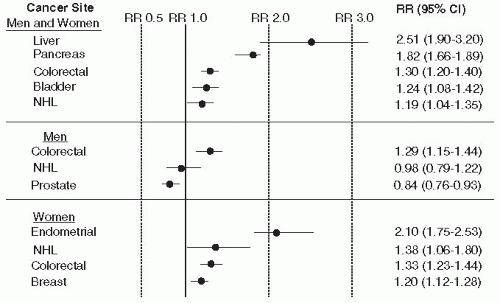
The association between diabetes and cancer was first reported in the 1960s.35 Accumulating evidence from case control and observational studies advocates an association between T2DM and cancer at multiple sites. The American Cancer Society Cancer Prevention Study II reported that, irrespective of BMI, adults with diabetes had a mortality risk from breast, colon, pancreatic, and liver cancers in excess of those without diabetes.36,37 Patients with diabetes have a 2-fold increased risk for developing cancers of the liver, pancreas, and endometrium, and a 1.2- to 1.5-fold likelihood of developing cancers of the colon, rectum, breast, and bladder (Fig. 8-4). Other cancers, such as those arising from the lung, do not appear to be associated with diabetes.35 The data on renal cell carcinoma, and non-Hodgkin lymphoma are inconclusive. Interestingly, few studies have explored the associated risks between T1DM and cancer. Only prostate cancer appears to have a lower risk in patients with T2DM. Although circulating testosterone levels have not been associated with prostate cancer, men with T2DM are generally noted to have reduced total and free plasma testosterone concentrations. The presence of diabetes also appears to increase the risk of all-cause mortality in patients with cancer.38
In 2007, 26 million Americans were estimated to be living with diabetes, whereas 12 million patients were receiving treatments for cancer.39 Approximately 25% of people living in the developed world succumb to cancer.40 Most patients present to their PCP with disease-state-specific symptoms. The PCP has the formidable task of determining if the individual has a benign or malignant disorder. PCPs are more experienced in diagnosing what is not cancer than counseling patients as to what metabolic, genetic, or lifestyle behaviors might adversely affect one’s future cancer risk. Assuming that primary care is the setting in which cancer is most often diagnosed, or at least suspected, the PCP should be at the forefront of performing routine presymptomatic oncologic risk assessments in patients regardless of their glycemic status. High-risk patients should be screened for cancer according to the evidence-based guidelines shown in Table 1-6 of the Introduction chapter. One should also assess each patient’s family history and modifiable risk factors (smoking, obesity, and alcohol use). Clinicians should be willing to comanage a cancer patient’s metabolic disorders in consultation with oncologic and surgical specialists.
Figure 8-4 • Results of a Meta-analysis of Cohort and Case-controlled Studies Examining Cancer Risk at Specific Sites in Patients with Diabetes. The dots represent relative risk and the bars represent 95% confidence intervals (CI). NHL, non-Hodgkin lymphoma. (Modified from Gallagher EJ, Fierz Y, Ferguson RD, et al. The pathway from diabetes and obesity to cancer, on the route to targeted therapy. Endocrine Pract. 2010;16(5):864-873.)
Relationship between Obesity, Diet, Physical Activity, Diabetes, and Cancer
Overweight individuals (BMI ≥ 30 kg per m2) have a higher cancer risk compared with those individuals having normal BMIs (18.5 to less than 25 kg per m2). The cancers most consistently associated with obesity are breast, colon, endometrium, pancreas, esophagus, gallbladder, kidney, liver, and prostate.35 Unfortunately, the positive benefits of intentional weight loss on reducing one’s risk of cancer are less certain. The Nurses’ Health Study did demonstrate a statistically significant inverse association between weight loss and postmenopausal breast cancer.41 The role of bariatric surgery in reducing cancer occurrence and mortality has not been established through prospective trials.
Diets that are low in red and processed meats but high in vegetables, fruits, and whole grains are associated with a lower cancer risk. Adding fiber to meals will protect against T2DM and improve insulin sensitivity.42,43 Physical activity may prevent colon, breast, and endometrial cancers while improving metabolic outcomes in patients with T2DM.35,44
Only gold members can continue reading. Log In or Register to continue
 Fixed, mottled, cyanotic limb
Fixed, mottled, cyanotic limb Ischemic, necrotic toes, with multiple erythematous granulating lesions on dorsum of foot (Note, most patients have no visual findings on examination)
Ischemic, necrotic toes, with multiple erythematous granulating lesions on dorsum of foot (Note, most patients have no visual findings on examination)