4 Chemical Modifiers of Radiation Response
This chapter deals with chemical agents that have been used solely as modifiers of radiation response and with methods to detect hypoxic cells in tumors. For a discussion of the interaction of cytotoxic cancer chemotherapeutic agents with radiation (actinomycin D, 5-fluorouracil, doxorubicin [Adriamycin], hydroxyurea, and paclitaxel [Taxol]), the reader is referred to Chapter 6.
Rationale for the Use of Radiosensitizers and Radioprotectors
Radiosensitizers
Radiosensitizers are compounds that, when combined with radiation, achieve greater tumor inactivation than would have been expected from the additive effect of each modality. The application of chemical agents that simply have an additive effect in normal tissues is equivalent to the administration of an increment of radiation dose with no differential benefit. The toxicities of the chemical agent and the radiation overlap with no major gain.1 The addition of a chemical modifier to a course of radiation to improve treatment results should be considered only in those tumor sites where there is already evidence that an increase in dose intensity by 20% to 30% will translate into an increase in tumor control, because most of the sensitizer enhancement ratios (SERs) are in the range of 1.2 to 1.3 (a 20% to 30% increase in the effective dose to the tumor). Examples of such tumors are head and neck tumors and carcinoma of the cervix, in which it has been demonstrated that there is a high fraction of hypoxic tumor cells and also a rapid cell turnover.2,3
Chemical Radiosensitizers of Hypoxic Cells and the Tumor Microenvironment
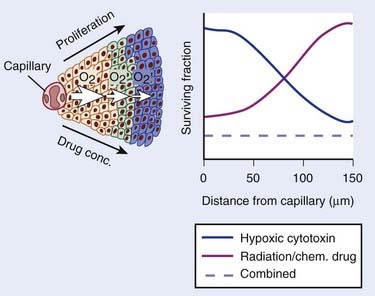
The role of the oxygen effect in promoting tumor cell inactivation by ionizing radiation has been well demonstrated in vitro and in animal tumor models for several decades. Mounting evidence of this influence in tumor control and patient survival has become available.2–7 Clearly, the microenvironment, the nutritional state of the tumor, and the presence of hypoxia are only some of the many factors that contribute to tumor radioresistance, and it is likely that this resistance is multifactorial, that is, caused by tumor hypoxia, proliferation rates, and inherent cell radioresistance, as well as other biologic microenvironmental factors such as the presence of cytokines. Nonetheless, the clinical data that hypoxia, by conferring radiation resistance, is a prognostic indicator of poor response to standard radiotherapy, at least for some tumors, is reasonably clear. Hypoxia, however, has other consequences beyond conferring radiation resistance. First, hypoxia causes cells to slow their rate of proliferation and to come out of cycle. Because most anticancer drugs are more effective against rapidly proliferating than slowly or nonproliferating cells, this slowing of cell proliferation leads to decreased cell killing in the hypoxic cells. In addition, because the concentration of anticancer drugs is higher closer to blood vessels than further away, both as a consequence of geometry and the reactivity of the drugs, there is less killing of the hypoxic cells, which are invariably the farthest from the blood vessels.
In summary, there are a number of well-established phenomena that cause a gradient of reduced cell killing by most anticancer agents as a function of distance from the vasculature (Fig. 4-1). Such a gradient has been shown in experimental tumors and in spheroid systems.8,9
Recent studies have also shown that hypoxia in solid tumors has an important consequence in addition to conferring a direct resistance to radiation and chemotherapy. Graeber and colleagues10 have demonstrated that low oxygen levels cause apoptosis in minimally transformed mouse embryo fibroblasts, and by selecting for mutant p53, might predispose tumors to a more malignant phenotype. Clinical data support this conclusion: Studies both with soft tissue sarcomas5 and with carcinoma of the cervix11,12 have shown that hypoxia is an independent and highly significant prognostic factor predisposing tumors to metastatic spread. Thus a more hypoxic tumor, in addition to being more difficult to control locally, is also more likely to have spread to distant sites and hence be more difficult to cure. In addition, hypoxia stabilizes the transcription factor HIF-1α, which increases levels of various survival factors such as vascular endothelial growth factor, which can protect against radiation damage to the tumor vasculature and hence, at least theoretically, protect the tumor from radiation damage.13,14
The rationale for developing hypoxic cell sensitizers has been based on the assumption that sensitizing hypoxic cells to radiation killing would improve the outcome of radiotherapy. The possibility of doing this was based on pioneering studies by Adams and Chapman and colleagues on the use of electron-affinic drugs to sensitize hypoxic bacteria and mammalian cells in vitro.15–17 The first drug of this class to show significant activity in sensitizing mouse tumors was the 5-nitroimidazole metronidazole, a drug that was already in clinical use.18,19 Data on this and other such compounds are discussed in the following text.
Nitroimidazole Compounds
Under hypoxic tissue conditions, electron-affinic nitroimidazoles oxidize the radiation-induced free radicals on deoxyribonucleic acid (DNA), thereby mimicking oxygen for the fixation of DNA damage. However, unlike oxygen, nitroimidazoles are not rapidly metabolized by the cells through which they penetrate and are thus able to reach areas beyond the oxygen-diffusion distance. They were shown by various groups to be effective in preclinical studies with transplanted mouse tumors in radiosensitizing the tumors to large single radiation doses without sensitizing normal tissues.20,21
The first compound to be investigated clinically in terms of oral and intravenous pharmacokinetics, toxicity, and efficacy in patients with solid tumors was metronidazole (a 5-nitroimidazole). The plasma β-half-life of the drug was 9.8 hours and the absolute oral availability was estimated to approximate 100%.19 The dose-limiting toxicity was manifested in gastrointestinal and peripheral neuropathic effects; therefore, this compound reached an estimated SER of only 1.2. Given this limitation, the first randomized control clinical trial of a hypoxic radiosensitizer showing efficacy was performed in patients with glioblastoma multiforme. This study demonstrated the relevance of tumor hypoxia in terms of patient survival, showing that the results with a less-than-optimal radiation fractionation regimen approached the level of the results obtained with conventional fractionation.22
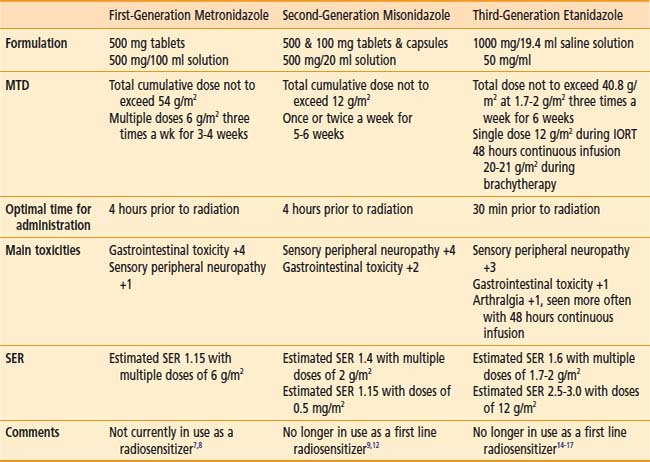
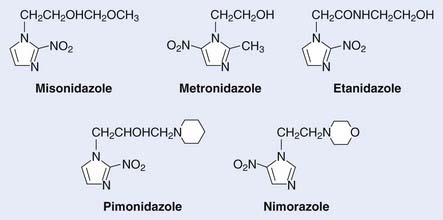
Of interest, a major spin-off of these early investigations with the pharmacokinetics of metronidazole, particularly the use of a high-dose intravenous route, was not in the field of oncology but in the practice of abdominal surgery and infectious diseases, in which the compound was used as a parenteral agent for anaerobic bacteria. These initial investigations prompted a level of high activity in the investigation of nitroimidazole compounds in human solid tumors and the search for new and better nitroimidazole compounds with less toxicity and higher SER. The first clinical studies on the second generation of these drugs, misonidazole, a 2-nitroimidazole, were initiated in both Europe and North America during the early 1980s (Table 4-1). The structures of the hypoxic sensitizers discussed are shown in Fig. 4-2.
Table 4-1 The Evaluation from First- to Third-Generation Nitroimidazole Compounds During the Past 25 Years
Misonidazole and Nimorazole
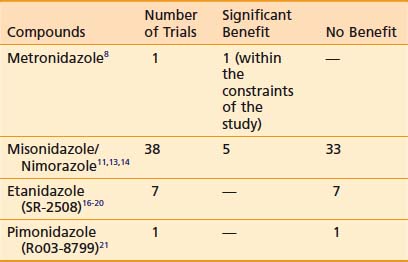
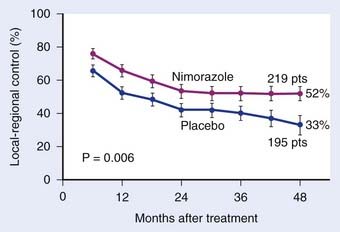
Misonidazole, a 2-nitroimidazole, was developed as a more efficient radiosensitizer because of its known increased electron affinity. In the oral form, the dose-limiting toxicity was again manifested in gastrointestinal effects (nausea, vomiting) and peripheral neuropathy, which limits the effective SER.23,24 Not surprisingly, almost all of the clinical trials of radiotherapy combined with misonidazole turned out to be negative,25 an outcome consistent with the small degree of radiosensitization expected with the clinically used low doses.26 Once more the inability to deliver a sufficient dose may have been one of the reasons that a significant proportion of large international clinical trials showed no benefit to misonidazole (Table 4-2). However, it has been shown that selected populations of patients with specific tumors did benefit by using this compound.27 This observation was made in patients with head and neck cancers. Overgaard and colleagues28 reported that not only with misonidazole but also with nimorazole (a 5-nitroimidazole), there was a significant benefit in a cohort of patients with stage T1 and T4 pharynx carcinoma in terms of local regional control (Fig. 4-3). Patients with hemoglobin levels lower than 9 mmol/L showed particular improvement. These two studies also showed that the compounds had a similar benefit, despite the fact that fewer fractions of radiation were “sensitized” in the misonidazole groups than in the nimorazole groups, in which the drug was administrated with every fraction of radiation (first 30 fractions). The significant improvement of the effect of the radiotherapeutic management of supraglottic and pharynx tumors was again demonstrated in a randomized double-blind phase III study of 414 patients receiving nimorazole or placebo in association with conventional primary radiotherapy (62-68 Gy, 2 Gy per fraction, 5 fractions per week).28 Of interest is that in this study the nimorazole could be given without major side effects. Nimorazole is currently standard treatment for patients in Denmark receiving radiation therapy for head and neck cancer.29 The benefit of misonidazole was not observed in another large clinical trial conducted in North America under the Radiation Therapy Oncology Group (RTOG) in patients with stage III and IV head and neck tumors, in which misonidazole was used with two of the five radiation fractions per week. In this study, the administration of the radiosensitizer was limited by neurologic complications, and the use of efficient doses was prevented.30 A prospective randomized trial was initiated afterward in the same cooperative group with a newer third-generation compound, etanidazole. A significantly greater dose of etanidazole than misonidazole could be administered for a sensitizer effect with acceptable gastrointestinal and neurologic toxicity.31
Etanidazole
Etanidazole (originally known as SR2508) was developed by a team led by Brown and Lee with the aim of reducing the neurotoxicity seen with misonidazole.31 It was postulated that because etanidazole is less lipophilic, it would be associated with a lower incidence of neuropathies. This was confirmed in a phase I pharmacokinetic and toxicity study in which doses three times higher than with misonidazole were delivered and fewer peripheral neuropathies were observed.31
Based on the encouraging results of the Danish Group in pharynx carcinoma with misonidazole and nimorazole, the RTOG initiated a two-part study in advanced head and neck cancer. The first part, a toxicity and logistic study in which etanidazole was used three times a week for 17 doses in combination with standard radiation, was completed with acceptable toxicity (although the 22% incidence of peripheral neuropathies seen in that study still presented a problem). Subsequently, a phase III study in a similar patient population and with the same frequency of sensitizer administration was completed in 1992. The results showed that adding etanidazole to conventional radiotherapy produced no benefit for patients with advanced head and neck carcinomas, except for a suggestion of benefit in a subset of patients with early stages (N0-N1 disease).32 A randomized study of 374 patients from 27 European centers, conducted between 1987 and 1990, adding etanidazole to conventional radiotherapy did not afford any benefit for patients with head and neck carcinoma. Furthermore the study failed to confirm the hypothesis of benefit for patients with early disease.33
A similar study in patients with locally advanced cancer of the prostate—T2b, T3, and T4—was also initiated in North America (RTOG). This study was designed to deliver the sensitizer with as many fractions of conventional radiation as possible. Nineteen doses of 1.8 g/m2 were delivered three times a week during the course of radiation, with tolerable toxicity. The results of this trial with regard to prostatic-specific antigen response and clinical disappearance of tumor are similar to those of historical control subjects, and are not considered to represent an improvement.34
Evidence exists that prolonged exposure to severe hypoxia can lead to increased sensitization beyond the oxygen effect, owing to the formation of reactive reduced metabolic species. Based on this evidence, an evaluation was made of etanidazole administered in 48-hour and 96-hour continuous intravenous infusions to patients undergoing brachytherapy.35 The use of etanidazole under these particular conditions is considered worth pursing.
Hypoxia marker studies (see the following text) that used 3H-misonidazole or 123I-iodoazomycin arabinoside showed evidence of tumor hypoxia in more than 50% of patients with small cell carcinoma (SCC) of the lung and indicated that tumor hypoxia could be one of the causes of chemoresistance and radioresistance in these patients. Therefore, a phase I and II clinical prospective study was initiated in patients with limited stage of small cell lung cancer, in which etanidazole was given in doses of 1.7 g/m2 three times a week with concomitant chemotherapy and thoracic irradiation. In patients with limited-stage disease, the median and the crude rates of survival at 5 years with no evidence of disease were superior to the best results reported in the literature from similar radiotherapy and chemotherapy regimens in which etanidazole was not used.36
Pimonidazole (a 2-nitroimidazole) was developed in Europe at the same time that etanidazole was developed as a third-generation sensitizer, and was considered to be more potent than misonidazole because of its potential to be concentrated in tumors as a result of its pH-dependent sidechain charge. The maximum tolerated dose, when administered with a daily 20-fraction course of radiotherapy, was established at 750 mg/m2. The dose-limiting toxicity has been in the central nervous system, manifesting as disorientation and malaise. A randomized clinical trial in advanced carcinoma of the cervix was conducted by 16 centers in Western Europe under the guidance of the Medical Research Council of the UK. Patient accrual was completed in May 1989. Overall and disease-free survival rates were found to be poor among the patients who received pimonidazole in combination with external radiation.37
Conclusions
The current status after  decades of clinical investigations with hypoxic cell sensitizers can be summarized by stating that these compounds have not become part of the standard practice of radiotherapy, at least in North America. In Denmark, however all head and neck cancer patients routinely are given nimorazole based on the positive phase III randomized trial of this drug with conventional radiotherapy.28 The only patients who appear to have benefited significantly from this approach are those with advanced pharyngeal and supraglottic carcinomas treated with radiation and either misonidazole or nimorazole. In the immediate future and with the advent of noninvasive markers of tumor hypoxia, it should be possible to select patients for the use of these agents. In addition, the increased use of stereotactic body radiotherapy is likely to make these compounds more attractive in the future because hypoxia is a bigger problem for large single or a limited number of large radiation doses and the individual doses of the particular sensitizers that can be delivered will be higher.
decades of clinical investigations with hypoxic cell sensitizers can be summarized by stating that these compounds have not become part of the standard practice of radiotherapy, at least in North America. In Denmark, however all head and neck cancer patients routinely are given nimorazole based on the positive phase III randomized trial of this drug with conventional radiotherapy.28 The only patients who appear to have benefited significantly from this approach are those with advanced pharyngeal and supraglottic carcinomas treated with radiation and either misonidazole or nimorazole. In the immediate future and with the advent of noninvasive markers of tumor hypoxia, it should be possible to select patients for the use of these agents. In addition, the increased use of stereotactic body radiotherapy is likely to make these compounds more attractive in the future because hypoxia is a bigger problem for large single or a limited number of large radiation doses and the individual doses of the particular sensitizers that can be delivered will be higher.
Possible Explanation for the Inconclusive Therapeutic Benefits Seen With Nitroimidazoles in Most Solid Tumors
Of interest is an updated review of all randomized clinical trials on approximately 10,108 patients combining tumor hypoxia modifiers (hyperbaric and normobaric oxygen plus carbogen and hypoxic radiosensitizers) with curative radiation, showing an improved effect of radiotherapy on local-regional control, without evidence of increase of radiation side effects in normal tissues.40
Current Status and Future Directions in Tumor Hypoxia
Microinvasive Methods of Measuring Tumor Hypoxia
One possible interpretation of the clinical sensitizer trials is that hypoxia is less important for the therapy of human tumors than for murine tumors and other model systems. Arguing against this is a series of studies using a newly developed semiautomatic needle electrode (Eppendorf Histograph).41–44 These studies not only confirm the radiation resistance of hypoxic human tumors, but demonstrate their more “aggressive” phenotype for other types of treatment failure (chemotherapy–resistance, metastasis, surgical). The overall “aggressiveness” of hypoxic tumors determined by this pioneering work is now much better understood since the discovery and subsequent elucidation of the central role played by hypoxia-inducible factor-1 (HIF-1) in many aspects of tumor behavior.45 The resolution of the Eppendorf system is roughly 0.7 mm and several assays capable of much finer resolution have been developed for immunohistochemical analysis.
Some of these microassays involve endogenous molecular changes (often HIF-mediated46) or inherent radiation resistance.47 The most extensively developed microscopic assay of hypoxia, also central to the development of noninvasive assays (see the following text), was based on the finding that 2-nitroimidazole metabolism led to the hypoxia-dependent formation of adducts between the metabolized drug (activated by nitro-reduction) and cellular macromolecules, later shown to be primarily thiol-containing proteins.48,49 Chapman first proposed that this metabolism could be used for the practical measurement of tissue hypoxia, and one resulting technique (autoradiography after excision of the labeled tumor) progressed to a clinical trial.50 The measurement of tritiated misonidazole metabolism by autoradiography was problematic for a general-use assay, but this problem was solved through the development of antibody-based assays for the detection of 2-nitroimidazole adducts, particularly using pimonidazole or EF5 as the hypoxia-detecting agent.51,52
One endogenous hypoxia marker currently capable of predicting outcome is carbonic anhydrase IX (CA-IX). CA-IX is one of several carbonic anhydrase enzymes, and is strongly upregulated under hypoxic conditions through the HIF-1α mechanism. CA-IX is expressed on the surface of cells and therefore can be detected by antibodies. However, its correlation with gold-standard measures of hypoxia is suboptimal.53
Noninvasive Methods of Measuring Tumor Hypoxia
Determination of therapy-relevant tumor hypoxia using nuclear medicine techniques holds many potential benefits, including timely stratification of treatment, prediction of outcome, and even the spatial optimization of radiation therapies using image-guided radiation therapy (IGRT), intensity-modulated radiation therapy (IMRT), and protons.54 It has become clear that the first of these is much more important than previously considered—that is, heterogeneity of the extent and degree of hypoxia between tumors or patients with otherwise similar characteristics can ultimately stifle the development and interpretation of hypoxia-specific therapies, resulting in the waste of clinical trial resources on patient cohorts for which the hypoxia-specific therapy is inappropriate. With the exception of Copper(II)-diacetyl-bis(N4-methylthiosemicarbazone) (Cu-ATSM) and the antibody developed against CA-IX, most agents being considered for the noninvasive detection of hypoxia are also 2-nitroimidazoles. Thus, it is fitting that the first agent developed for noninvasive imaging of hypoxia [18F]fluoromisonidazole (18F-FMISO) was first used to demonstrate the predictive value of the first clinically developed hypoxic cell cytotoxin (tirapazamine [TPZ]).55,56 Nevertheless, this delay in the successful application of 18F-FMISO imaging has resulted in the extensive development of other possible noninvasive hypoxia markers.
Half-Life of Isotope versus Drug
Chapman and colleagues17 suggested that the relatively short isotope half-life of 18F (≈110 minutes) was suboptimal in detecting tumor hypoxia because, first, this does not allow adequate clearance (pharmacologic half-life of drug) of nonmetabolized drug (which forms the image background), and second, binding to hypoxic cells should increase with time, so that inherent limitations exist in generating optimal tumor versus normal tissue contrast during the relatively short imaging times suitable for 18F.57 Use of iodine as the detecting isotope was considered superior because of its variety of half-lives and decay types. However, directly iodinating the imidazole ring of misonidazole did not lead to suitably stable compounds, so a variety of nucleoside derivatives were devised, with the iodine conjugated to the sugar moiety rather than the 2-nitroimidazole. These compounds (exemplified by iodoazomycin arabinoside [IAZA] and iodoazomycin galactopyranose [IAZGP]) were also more polar than FMISO (see next paragraph). Both single photon emission computed tomography (SPECT) (138I) and positron emission tomography (PET) (139I) isotopes have been used to evaluate the utility of these drugs. Clinical trials of IAZA successfully imaged hypoxia but because of deiodination this agent was not considered optimal.57 IAZGP is under current investigation clinically at the Memorial Sloan Kettering Institute. Although the positive aspects of longer-lived isotopes seem clear, there are also negative aspects that must be mentioned. First, to provide a suitable image quality, the number of counts and imaging time must be specified. For these to be equivalent for long- versus short-lived isotopes, the former must necessarily cause a substantially higher total radiation dose burden to the patient. This is exaggerated for many PET isotopes (e.g., Cu and I), because the fraction of positron emissions per decay can be much less than one. This problem cannot be resolved by use of SPECT isotopes, because, other factors being equal, SPECT imaging has an inherently lower resolution than does PET imaging. Ultimate resolution of PET depends on the energy spectrum of the positron, and 18F is optimal in this respect.
Drug Polarity (Octanol-to-Water Partition Coefficient)
Because of the potential high resolution and low patient radiation dose from 18F, several other fluorinated drugs have been developed. Some of these compounds have been significantly more polar than FMISO. The goal of minimizing neurotoxicity seems “off-target” for the use of noninvasive imaging agents, because their concentration is orders of magnitude lower than was used in the sensitizer trials. Additionally, there are data suggesting that highly polar nitroimidazoles do not achieve suitable access to brain and possibly other tissues.58 Thus, it is possible that polar imaging agents will have to be evaluated much more thoroughly with respect to their biodistribution and ability to diffuse into actively metabolizing tissue.
Drug Biodistribution and Stability
EF5’s design was based on specific properties of oxygen dependence of bioreduction, drug stability, and biodistribution determined in former pharmacologic and biochemical studies. It was hypothesized that emphasis on the uniform biodistribution allowed by a lipophilic molecule, in effect minimizing excretion, might allow relatively low hypoxia-dependent bioreduction to be detected above the uniform background of the parent drug.59 These properties were validated at the relatively high concentration used for immunohistochemistry (≈100 µm—using monoclonal antibodies against EF5 adducts) and appear to be maintained at approximately 1000-fold lower drug concentrations used for PET.60 Recently, two other 18F-containing hypoxia markers have been tested in humans: [18F]fluoroazomycin arabinoside,61 the fluorinated equivalent of IAZA; and EF3,62 a tri-fluoro analog of EF5. These drugs are somewhat more lipophilic than FMISO, with octanol-to-water partition coefficients close to 1.
Several imaging agents have been found to concentrate in tumors, but their precise mechanism binding is not fully understood. The best characterized of these is Cu-ATSM. ATSM is a copper chelator related to the perfusion marker copper pyruvaldehyde bis (N4-methylthiosemicarbazone).63 ATSM is very lipophilic but unexpectedly shows rapid biodistribution and binding. Like iodine, copper has a number of radioactive isotopes with selectable properties. Thus this hypoxia marker has many appealing properties.
Manipulation of the Tumor Microenvironment
Increasing the Oxygen-Carrying Capacity of Blood: Hyperbaric Oxygen and Fluosol
Clinical studies have been completed in which hyperbaric oxygen,64 carbogen,65 packed red cell transfusions,66,67 and oxygen-carrier substances such as perfluorocarbons (Fluosol-DA) have being used.68,69 Although the use of the hyperbaric oxygen chamber at three atmospheres presented technical difficulties, such as barotrauma and the limitations of its use to only a few high-dose fractions of radiation, 3 out of 10 clinical trials showed significant positive results. The beneficial effect was seen particularly in patients with advanced cancer of the head and neck and of the cervix.70
A phase II study of Fluosol-DA and 100% oxygen in combination with radiotherapy in advanced head and neck tumors has shown promising results.68,69 Investigators have also been assessing the compound 2-(4-[{3,5-dimethylanilino}carbonyl]methyl]phenoxy)-2-methylproprionic acid derivative, an allosteric hemoglobin modifier, and preliminary reports are encouraging.71





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


