Case 9
Presentation
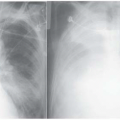
A 66-year-old woman is referred by her primary care physician for further workup of a left lung mass. She is a former smoker, having quit in 1994. She has noted increasing shortness of breath and cough for 6 weeks, but no hemoptysis. She quit work 3 weeks ago because of increasing fatigue, and she has lost 8 pounds over the last month.
Differential Diagnosis
There is little doubt that this patient has a malignancy, although sometimes a smoldering infection such as tuberculosis (TB) or an empyema can cause similar fatigue and weight loss. The symptoms of cough and shortness of breath suggest airway compression, and thus suggest lung cancer as opposed to a primary mediastinal tumor or a pleural process. The rapidity of progression of her symptoms suggests this is a rapidly growing tumor, such as small cell lung cancer (SCLC). In addition to detailed evaluation of the clinical presentation, a computed tomography (CT) scan of the chest is helpful. The clinical findings and the radiographic characteristics generally allow a presumptive diagnosis to be made, and furthermore, usually define which tests are needed for further workup with regard to diagnosis and staging.
Recommendation
The patient should have a complete history and physical examination, and a chest CT scan.
Case Continued
A careful history discloses no other symptoms. Specifically, she denies any neurological symptoms such as headaches or focal weakness, and has no new bone or joint pains. Past medical history, family history, social history, and review of systems are unremarkable except for smoking and that her father died of lung cancer. Her physical examination is entirely normal. Notably, there are no palpable supraclavicular lymph nodes.


Differential Diagnosis Continued
The combination of risk factors and the radiographic appearance leave no real doubt that this is a lung cancer. The epicenter of this tumor is in the left lung, although it extends dramatically into the middle mediastinum. The rapid progression of symptoms, the central nature of the tumor, and the bulky mediastinal involvement makes SCLC very likely.
Other possible diagnoses include a non-small cell lung cancer (NSCLC), a lymphoma, or a mediastinal germ cell tumor. This tumor could be a NSCLC, although these typically have a less central epicenter and less dramatic mediastinal involvement. Although mediastinal germ cell tumors are more common in younger patients, they do occur in this age group and may be rapidly growing. However, they are typically centered in the anterior mediastinum, and the radiographic appearance of this case would be highly unusual. Lymphoma may also exhibit rapid growth, but that presentation is more common in the pediatric population and young adults. Furthermore, patients with lymphoma usually have palpable nodes in extrathoracic sites and additional areas of nodal enlargement on CT (in the anterior mediastinum, lower mediastinum, opposite hilum, neck, axilla, or upper abdomen).
This patient has nonspecific symptoms of distant metastases (fatigue and weight loss), although she does not have organ-specific symptoms (neurologic or skeletal). The physical exam does not suggest an obvious site of distant metastases that would be easy to biopsy and thereby confirm both the diagnosis and the stage.
Discussion
Approximately 15% to 20% of lung cancers are classified as SCLC. Approximately 2% to 3% of these cases have a mixed SCLC and NSCLC histologic pattern. SCLC is characterized by rapid growth and early involvement of mediastinal nodes and distant metastatic sites. The primary risk factor for SCLC is tobacco consumption. In fact, the occurrence of SCLC in a nonsmoker is so rare (0% to 3%) that one must question the diagnosis of SCLC in a patient who is a lifelong nonsmoker.
Signs and symptoms of SCLC relate to the bulk of disease and anatomic location of the tumor. In a population-based retrospective review of presenting symptoms, cough, weight loss, dyspnea, and chest pain were each present in approximately one third of patients with SCLC. Hemoptysis and hoarseness also occur frequently. Regional and mediastinal lymphadenopathy are present in the vast majority of patients. Various paraneoplastic syndromes have been reported with SCLC. These include the syndrome of inappropriate antidiuretic hormone (SIADH), hyponatremia, ectopic adrenocorticotropic hormone (ACTH) production, and Eaton-Lambert syndrome.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


