Case 88
Presentation
A 53-year-old woman presents complaining of a 3-month history of fatigue, abdominal bloating, and persistent abdominal swelling such that she notes that her clothes do not fit. She has had a modest weight gain of about 10 pounds. She has noted some constipation but no pencil stools or melena. She has noted some mild nausea and decrease in appetite along with early satiety, but she denies emesis. Her family history is significant for a sister with breast carcinoma, diagnosed at the age of 47. A paternal aunt also has had breast cancer, at unknown age at diagnosis.
The abdominal examination shows moderate abdominal distension, with no enlarged liver or spleen, but there is a suspicion of a mass in the midepigastrium and there is a fluid wave. Pelvic examination shows normal external genitalia, bladder, urethra, and vagina. The cervix is grossly normal, and a Papanicolaou test is collected. On bimanual examination, there is a firm mass filling the cul-desac, not freely moveable, measuring about 15 cm in diameter. Rectovaginal examination shows the rectum to be deviated toward the right and densely adherent to this mass. Results of fecal occult blood tests (stool guaiac) are negative.
Differential Diagnosis
The differential diagnosis must include an adnexal neoplasm (benign, borderline, malignant, or metastatic), infectious causes such as tubo-ovarian abscess, appendiceal abscess, or diverticular abscess, uterine fibroid, or advanced bladder or colon neoplasm.
Discussion
Some relevant clues are revealed during this patient’s history. Ovarian cancer does not have a pathognomic set of symptoms, but there are quantitative differences between the symptoms of healthy women attending a primary care clinic and women found to have ovarian carcinoma.
Ovarian cancer has often been called the “silent killer” because pathognomic symptoms are not recognized until late in the course of the disease. Recent data suggest that there are symptoms that antedate, often by several months, the diagnosis of ovarian cancer. These symptoms are not limited to women with advanced-stage ovarian cancer, thus offering some hope that early identification of telltale symptoms may help diagnose this lethal disease at an earlier, more treatable stage. The most common symptoms of ovarian cancer include bloating, increasing abdominal girth, abdominal pain, urinary urgency, and pelvic pain. The combination of bloating, increased abdominal size, and urinary urgency occurs in about half of ovarian cancer patients but in < 10% of patients attending primary care clinics. The symptoms are noted to be more severe and of shorter duration among women with ovarian cancer.
The family history in this patient is also worthy of further notice. Her sister and paternal aunt both suffered from breast cancer, and the sister was diagnosed at an early age. This family history is associated with an increased risk of carrying a BRCA1 or BRCA2 mutation within the family. This risk is substantially increased if ovarian cancer is also present within the family. Based upon her family history, the patient should be offered genetic counseling and testing for mutations in BRCA1 and BRCA2 if appropriate.
Her physical examination documents a palpable adnexal mass along with ascites and, possibly, a mass in the omentum. These findings mandate further evaluation. Testing for the CA 125 tumor marker should be ordered and an imaging study should be obtained. In cases in which the clinical suspicion of ovarian cancer is high, a computed tomography (CT) scan of the abdomen and pelvis is superior to an ultrasound. The CT scan allows evaluation of the retroperitoneal nodes, omentum, pancreas, liver, spleen, kidneys, and adrenals. Additionally, neoplasms of the stomach or colon are occasionally identified through critical evaluation of the CT images. Conversely, where the clinical suspicion of ovarian carcinoma is low, an ultrasound
provides an inexpensive, low-risk method of characterizing an adnexal mass.
provides an inexpensive, low-risk method of characterizing an adnexal mass.
Case Continued
CA 125 level is elevated at 792.
▪ CT Scans
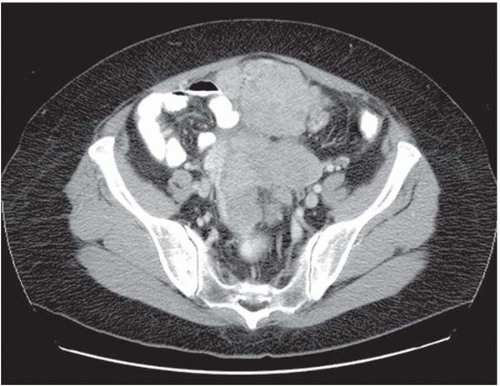 Figure 88.1A |
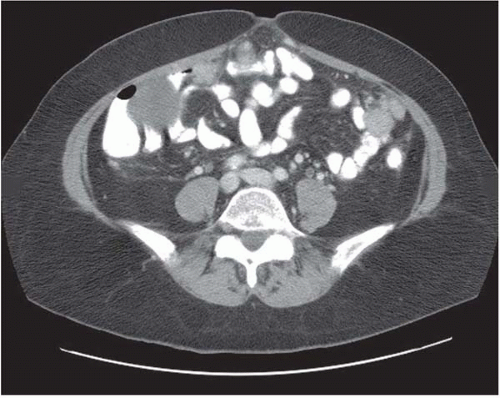 Figure 88.1B |





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


