Case 86
Presentation
A 63-year-old woman is referred for further evaluation of a 3-week history of urinary frequency and intermittent gross hematuria. She is a 30-pack-year smoker and has no significant past medical or surgical history. Physical examination is unremarkable. Serum creatinine is 0.7 mg/dL, hematocrit 35%, and alkaline phosphatase and liver enzymes are within the normal range. Urinalysis and culture are significant only for hematuria at this time. An abdominal and pelvic computed tomography (CT) scan is performed.
▪ CT Scan
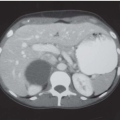
 Figure 86.1 |
CT Scan Report
Filling defect within urinary bladder. There is no hydronephrosis or pelvic/retroperitoneal adenopathy. No urinary calculi are visualized.
Differential Diagnosis
The differential diagnosis for hematuria can be quite extensive. Associated symptoms may aid in distinguishing the etiology, such as flank pain for nephrolithiasis and frequency or dysuria for cystitis. Painless gross hematuria is the classic symptom for bladder cancer, although irritative voiding symptoms are not uncommon especially when carcinoma in situ is present. Hematuria, either gross or microscopic, is noted in over 60% of bladder cancer cases, and therefore, upper tract imaging (intravenous pyelography, CT scan, and ultrasound) and lower urinary tract inspection via cystourethroscopy are essential to rule out malignancy.
Discussion
Transitional cell carcinoma (TCC) of the bladder is the second most common malignancy of the genitourinary tract and the second most common cause of death among genitourinary tumors. Although more common in men (ratio of 2.7:1), it remains a considerable source of morbidity and mortality in women. Approximately 80% of patients with primary TCC will display a relatively indolent, low-grade tumor confined to the superficial mucosa. Most of these patients are managed with transurethral resection and selective administration of intravesical chemotherapy or immunotherapy. Despite the relatively “benign” nature of superficial TCC, the recurrence rate can be as high as 70%, thus necessitating frequent costly long-term follow-up. In addition, up to one third of recurrent superficial tumors may eventually progress to a higher grade and/or stage. Muscleinvasive tumors are diagnosed de novo in 15% to 30% of all bladder cancer patients. Unlike superficial disease, invasive TCC typically displays a highly aggressive behavior, as exemplified by the fact that nearly 50% of patients undergoing definitive local therapy for invasive tumors relapse with distant metastases within 2 years of treatment. Clearly, TCC represents a heterogeneous entity with significant malignant potential.
The gold standard for diagnosis of bladder cancer is cystoscopy with transurethral resection of the bladder tumor (TURBT). This allows histopathologic sampling of the tumor and can also be therapeutic for small superficial lesions. Further therapy depends
on the histologic cell type, tumor grade, and pathologic stage, which are determined from the transurethral resection.
on the histologic cell type, tumor grade, and pathologic stage, which are determined from the transurethral resection.