Case 85
Presentation
A 53-year-old man with no significant past medical history is referred to your office with a 1-month history of intermittent gross hematuria and left flank pain. He is a nonsmoker and has had no prior surgeries. Physical examination is notable only for a palpable left upper quadrant abdominal mass. His serum creatinine is 1.1 mg/dL, hematocrit is 35%, and liver function tests, coagulation panel, and prostate-specific antigen level are normal. Urinalysis and culture show no evidence of infection. An abdominal computed tomography (CT) scan is obtained.
▪ CT Scan
 Figure 85.1A |
 Figure 85.1B |
CT Scan Report
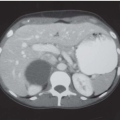
Large left renal mass with tumor thrombus extension into left renal vein and inferior vena cava.
Differential Diagnosis
The differential diagnosis for a renal mass in an adult can be broadly divided into benign (simple cyst, angiomyolipoma, oncocytoma) and malignant (renal cell carcinoma, sarcoma, metastasis) tumors. In light of a venous tumor thrombus, renal cell carcinoma should be the primary diagnosis.
Discussion
Renal cell carcinoma (RCC) is the most common malignant tumor of the kidney. Despite the increased incidence of small incidentally detected renal lesions, locally advanced tumors also continue to be diagnosed with increasing frequency. Of patients with RCCs, 4% to 10% demonstrate direct tumor extension into the vena cava. This form of tumor growth tends to be by expansion along the pathway of least resistance rather than by direct invasion, thus the vein wall itself is rarely involved. Most contemporary series have shown that tumor thrombus extension does not necessarily carry an ominous prognosis provided that complete surgical resection can be accomplished, and that there is no associated perinephric fat involvement, invasion of contiguous visceral structures or regional lymph nodes, or distant metastatic sites. Five-year survival rates for patients with vena caval extension without evidence of metastatic disease have been reported to be 30% to
70% following radical nephrectomy and tumor thrombectomy. Controversy exists regarding the prognostic significance of the level of vena caval tumor thrombus extension. The surgical management of RCC with tumor thrombus extension remains a technically challenging endeavor. Preoperative assessment of the cephalad extent of the thrombus is critical in planning the surgical approach. To that extent, magnetic resonance imaging (MRI) and transesophageal echocardiography are now commonly utilized in the preoperative planning.
70% following radical nephrectomy and tumor thrombectomy. Controversy exists regarding the prognostic significance of the level of vena caval tumor thrombus extension. The surgical management of RCC with tumor thrombus extension remains a technically challenging endeavor. Preoperative assessment of the cephalad extent of the thrombus is critical in planning the surgical approach. To that extent, magnetic resonance imaging (MRI) and transesophageal echocardiography are now commonly utilized in the preoperative planning.
Recommendation
Staging evaluation and MRI of chest and abdomen. Transesophageal echocardiogram to assess level of tumor thrombus.
Case Continued
Chest x-ray and bone scan show no evidence of metastatic disease.
▪ MRI
 Figure 85.2A |
 Figure 85.2B
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|