Case 83
Presentation
A 35-year-old man with no significant past medical history notices a right hemiscrotal mass on self-examination. The mass is painless, firm, and apparently intratesticular. The primary medical doctor orders a scrotal ultrasound and refers the patient to you.
▪ Ultrasound Image
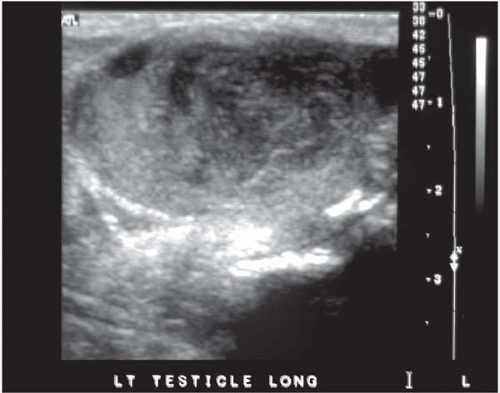 Figure 83.1 |
Ultrasonography Report
On ultrasound, the right testis and adnexal structures are normal. The left testis exhibits a solid hypoechoic intratesticular mass.
Differential Diagnosis
Most solid intratesticular masses represent germ cell testicular cancer. Two basic types exist: seminomas and nonseminomas. Seminoma is the most common single type, whereas nonseminomas typically consist of various components (embryonal carcinoma, yolk sac tumor, teratoma, and choriocarcinoma). Other possibilities include Leydig and Sertoli cell tumors, most of which behave in a benign fashion. Another possibility is an epidermoid cyst, which is a monolayer teratoma and is a benign lesion. In older men, lymphoma would be another consideration. Intratesticular inflammatory conditions are extremely
rare, and a patient who presents with the ultrasound described in this case presentation usually has a tumor.
rare, and a patient who presents with the ultrasound described in this case presentation usually has a tumor.
Recommendation
This patient should have a determination of serum alpha-fetoprotein, beta human chorionic gonadotropin (HCG), and lactate dehydrogenase (LDH). Approximately 10% of seminomas have a low-level elevation of beta HCG; an elevation of serum alpha-fetoprotein is synonymous with the diagnosis of nonseminoma. An elevation of serum LDH is not diagnostic but may aid in following the response to therapy.