Case 82
Presentation
The patient is a 79-year-old white male with a past medical history significant for repair of an abdominal aortic aneurysm, endovascular repair of a thoracic aneurysm, coronary artery disease, and carotid vascular disease. He was found 1 year ago to have an incidental 4.0-cm right adrenal mass on a computed tomography (CT) scan. The CT scan was performed for follow-up evaluation of his thoracic aneurysm. The patient was completely asymptomatic at the time, and underwent serum and urine cortisol tests as well as serum electrolyte and catecholamine tests, which were all negative.
The patient now presents to your office with a follow-up CT scan showing an increase in the size of the right adrenal mass and some right flank pain.
▪ CT Scan
 Figure 82.1A Copyright © 2004 Lahey Clinic. |
 Figure 82.1B Copyright © 2004 Lahey Clinic. |
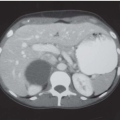
CT Scan Report
A large 6 × 5.8-cm right adrenal mass is present, adjacent to a large aortic aneurysm. The mass does not appear to invade any surrounding structures, and a clear plane between the adrenal mass and the kidney exists. Multiple simple cysts are present in both kidneys. A large thoracic and abdominal aneurysm is evident
Differential Diagnosis
The differential diagnosis for adrenal masses includes adenomas, pheochromocytomas, myelolipomas, ganglioneuromas, adrenal cysts, hematomas, cortical carcinomas, and metastasis from other cancers.
Discussion
With the increase in the utilization of abdominal imaging techniques, such as ultrasonography and CT scanning, there has been a dramatic increase in incidentally discovered adrenal masses, also known as incidentalomas. Solid adrenal masses, regardless of symptoms, should undergo biochemical assessment and appropriate radiologic imaging.
In patients with a prior history of cancer, up to three fourths of asymptomatic adrenal masses will prove to be metastases. In cases of prior malignancy, a needle biopsy may be warranted. In patients with no history of cancer, two thirds of these tumors are benign lesions. The size of the adrenal mass is clinically important because the prevalence of adrenal cortical carcinoma is related to size. Although adrenal carcinoma accounts for <5% of all adrenal masses smaller than 4 cm, they can account for 25% of all adrenal lesions larger than 6 cm. Some series have demonstrated that over 90% of all adrenal carcinomas are 6 cm or larger.
Biochemical or hormonal evaluation includes 24-hour urine cortisol levels and determination of fractionated urinary and/or plasma metanephrines. Plasma-free metanephrines are also important because they are highly sensitive for detecting pheochromocytomas. In patients with hypertension, a potassium level and a plasma aldosterone concentration-plasma renin activity ratio should also be determined. Glucocorticoid evaluation should only be performed if Cushing syndrome or virilization are clinically evident.
Proper radiologic imaging with either CT scanning or magnetic resonance imaging (MRI) is necessary. As previously mentioned, adrenal malignancies are almost always larger than 6 cm, and CT scans provide a relatively accurate assessment of tumor size. CT scans are also useful for distinguishing benign lesions such as myelolipomas and cysts from malignant lesions.
MRI is also a valuable diagnostic tool, especially for tumors <5 cm. On T1-weighted images, most benign adenomas appear hypointense or isointense in relation to the spleen or liver, with little change in intensity on T2 images. Adrenal cortical carcinomas, however, are felt to be hypointense to the liver or spleen on T1 mages but hyperintense on T2 images in relation to the liver or spleen. This finding, however, is not exclusive to adrenal cortical carcinomas because neural tumors, metastatic tumors, hemorrhage, and other lesions also have similar findings.
Newer applications of existing technologies, such as CT and MRI, as well as alternative studies, such as NP59 scanning, are enabling greater accuracy in differentiating between benign and malignant lesions.
There is little role for fine-needle aspiration (FNA) of adrenal masses unless a prior or concomitant history of cancer exists. The most common primaries that metastasize to the adrenal include melanoma, and lung, breast, and colon cancer.
In general, surgical extirpation is required for hormonally active adrenal lesions, for biochemically inactive adrenal lesions larger than 6 cm, and for adrenal lesions that grow in size or have radiographic evidence consistent with malignancy.
Recommendation
Anatomical imaging with MRI. Hormonal evaluation with 24-hour urine cortisol, serum catecholamines, and serum cortisol. Vascular surgery consultation is necessary to evaluate the stability of his aneurysms and determine a possible connection between the aneurysms and his recent right flank pain.