Case 8
Presentation
The patient is a 61-year-old man who is having knee-replacement surgery. His medical history includes osteoarthritis, mild hypertension, chronic obstructive pulmonary disease, and gastroesophageal reflux disease. He has no surgical history. His medications are a beta-blocker, some inhaled bronchodilators, a proton-pump inhibitor, and a COX-2 inhibitor. He has a 90-pack-year smoking history, and drinks alcohol occasionally. He reports an intermittent chronic cough. He has had no hemoptysis, hoarseness, chest pain, dyspnea, or facial swelling. On physical examination, pertinent findings include globally decreased breath sounds and mild expiratory wheezes. There is no dullness to chest percussion. The remainder of his physical exam is unremarkable. He brought his chest radiograph with him.
▪ Chest X-Ray
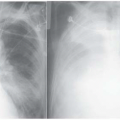
 Figure 8.1 |
Chest X-Ray Report
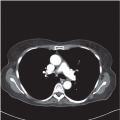
There is a suspicious nodule in the left upper lobe, but otherwise lung fields are clear.
Differential Diagnosis
The most likely diagnosis of a newly identified lung mass in a 61-year-old smoker is non-small cell lung cancer (NSCLC). This is the working diagnosis until definitively excluded. When definitively excluded, alternative diagnoses can be considered, including infection, benign tumors, and metastatic disease.
Discussion
A primary lung cancer can be definitively diagnosed using four methods: sputum cytology, flexible bronchoscopy, transthoracic needle aspiration (TTNA), and at operation. Sputum cytology carries a sensitivity of 66% and specificity of 99% when done at an institution with a well-established sputum cytology program, but is rarely performed now. Reports of flexible bronchoscopy vary by tumor location. The sensitivity for central tumors is reported to be about 88%, but falls to 69% or less for peripheral tumors. Thus, nondiagnostic results of bronchoscopy for a peripheral lesion that is suspicious for cancer do not obviate the need for further evaluation. The sensitivity of TTNA is reported to be as high as 90%, but the false-negative rate is generally found to be between 20% and 30%. Thus, a nondiagnostic TTNA also does not exclude cancer. Its role in the workup of suspicious lesions is debatable because the results will not affect therapy if the patient is an acceptable candidate for lung resection. Either outcome—identifying cancer or leaving it not disproved—will lead to surgical resection. Exhaustive efforts to obtain definitive tissue diagnosis should be used in cases where neoadjuvant (preoperative) therapy is planned or surgery is not feasible. Patients with suspicious tumors, clinically early-stage disease, and those who are candidates for surgery should have appropriate surgical therapy, despite a nondiagnostic TTNA or bronchoscopy.
Recommendation
Flexible bronchoscopy.
Case Continued
Based on the likelihood of NSCLC, a flexible bronchoscopy is performed, but no abnormalities are seen. Results of bronchial brushings and washings are also negative. A TTNA is considered, but is not performed for the reasons outlined perviously; the results, diagnostic or not, would not alter the plan of treatment for this patient.
Diagnosis and Recommendation
Highly likely NSCLC. A thorough history and physical examination complemented with appropriate staging (computed tomography [CT] scan, positron emission tomography [PET] scan, mediastinoscopy) of the tumor is important in the treatment of lung cancer.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


