Case 79
Presentation
A 25-year-old woman presents to the emergency room complaining of headache, palpitations, and anxiety. She has had similar symptoms several times over the past 3 months. On physical examination her blood pressure is 210/120 mm Hg in both arms and she is noted to have an enlarged thyroid. Chest x-ray is within normal limits. Complete blood cell (CBC) count and chemistry profile are unremarkable.
Differential Diagnosis
The differential diagnosis of hypertensive crisis in a young woman includes essential hypertension, stimulant abuse, renal artery stenosis, hyperthyroidism, pre-eclampsia, and pheochromocytoma.
Discussion
The episodic nature of the “spells” described by the patient suggests the possibility of pheochromocytoma. This is best evaluated by biochemical studies including plasma and/or urinary catecholamines and metanephrines. These tests take several days to return, and therefore computed tomography (CT) or magnetic resonance imaging (MRI) of the adrenal glands is the quickest test to evaluate for the presence of adrenal pheochromocytoma.
Recommendation
CBC, electrolytes, thyroid function tests, drug screen, pregnancy test, and CT scan of the abdomen.
Case Continued
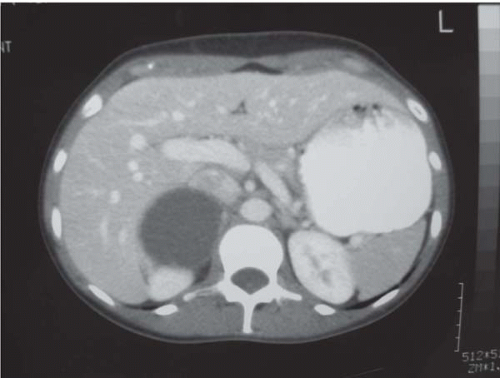
The patient has a normal CBC and electrolytes, negative pregnancy test, normal thyroid functions (T4 and TSH), and negative drug screen. CT of the abdomen shows a 7-cm cystic mass in the right adrenal. Plasma metanephrines are elevated. Twenty-four-hour urine normetanephrine is 30 nmol/L (normal is <1 nmol/L), 24-hour urine metanephrine is 5 nmol/L (normal is <0.5 nmol/L), and 24-hour urine epinephrine and norepinephrine are elevated as well.
Diagnosis and Recommendation
Right adrenal pheochromocytoma. Adrenalectomy is recommended, with preoperative preparation with alpha-blockade. The presence of a pheochromocytoma coexisting with a thyroid mass raises the possibility of multiple endocrine neoplasia (MEN) type 2a with medullary thyroid carcinoma (MTC). Measurement of serum calcitonin level and fine-needle aspiration (FNA) cytology of the thyroid mass are recommended after removal of the pheochromocytoma.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


