Case 66
Presentation
A 59-year-old man with no previous medical history complains of persistent dull abdominal pain that extends to the perineum. He reports that his bowel function has worsened slightly over the last couple of years. On rectal examination, a firm mass is palpable on the posterior aspect of the rectal ampulla; the superior margin of the mass is not appreciable. On neurologic examination, S2-S3 dysesthesia is detected. The patient has already undergone an abdominal ultrasound showing a presacral solid mass.
Differential Diagnosis
Metastatic tumor is the most frequent sacral lesion, particularly in adults older than 30 years, and should be excluded primarily. Among primitive sacrococcygeal masses, chordoma is the most frequent malignant disease, and the most common benign lesion is giant cell tumor.
Discussion
Among sacral primary tumors, 40% are chordomas, 12% are giant cell tumors, 8% are myelomas, 8% are lymphomas, 8% are Ewing sarcomas, 5% are chondrosarcomas, 4% are osteosarcomas, 4% are fibrosarcomas, and 3% are aneurysmatic bone cysts.
Chordoma is a rare neoplasm arising from aberrant primitive notochord remnants, localized to the midline spine, in the sacrococcygeal region and at the skull base. Tumor burden ranges from 2 to 30 cm maximum diameter at diagnosis. Symptoms are nonspecific, median age of presentation is 50 to 60 years, and there is a male predominance.
Recommendation
Biopsy to establish tissue diagnosis is recommended.
Discussion
Transrectal needle biopsy should be avoided (unless a rectal resection has already been planned) due to possible neoplastic seeding of the pelvis and viscera. Transperitoneal surgical biopsy must be avoided as well. Computed tomography (CT)-guided fine-needle biopsy or core needle biopsy by a posterior approach should be discussed with the operating surgeon, and the biopsy site should be tattooed. If needle biopsy is not feasible or the material obtained is not sufficient, surgical biopsy is indicated, with posterior small midline access to permit subsequent excision of scar.
Diagnosis and Recommendations
Chordoma. Complete staging with abdominopelvic magnetic resonance imaging (MRI) and CT scan of the chest to evaluate local extent of disease and presence of metastases.
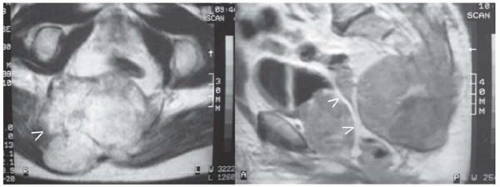
▪ MRI
 Figure 66.2 A B |
MRI Report
Axial T2 MRI (A) reveals an expansive pelvic mass measuring 12 × 12 cm involving the higher sacral vertebrae and coccyx. The rectum is displaced anteriorly without any evidence of invasion. There is posterior and caudal extension of the lesion toward the buttocks with muscle infiltration bilaterally. (B) On sagittal T1, bone structure is disrupted, and the rectum is displaced by tumor mass.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


