Case 63
Presentation
The patient is a 42-year-old woman complaining of vague lower abdominal pain for approximately 4 to 6 months with a recent increase in pain and left thigh sciatica. There is no history of trauma to the anatomical region. There are no systemic symptoms such as weight loss, anorexia, or fever. Physical examination reveals a large mass in the lower portion of the abdomen. The patient’s abdomen appears obviously distended and a 10 × 20-cm mass is palpated. This nontender mass is quite firm and appears fixed to the underlying left pelvis. A pelvic examination shows a large extravaginal mass to both the right and left sides of the uterus. The ovaries are not palpable. Neurological examination reveals no evidence of neuropathy, although there is a positive straight leg raising sign on the left side. There is no sensory or reflex loss appreciated in this extremity. Her history is negative for other gastrointestinal or genitourinary complaints, and she is not pregnant.
Recommendation
Plain radiograph of the pelvis, computed tomography (CT) scan and magnetic resonance imaging (MRI) of the pelvis are recommended.

▪ CT Scan
 Figure 63.2A |
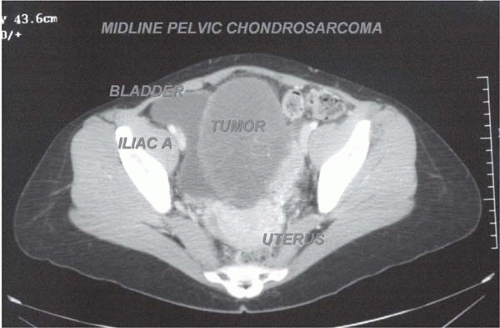 Figure 63.2B |
Pelvic X-Ray Report
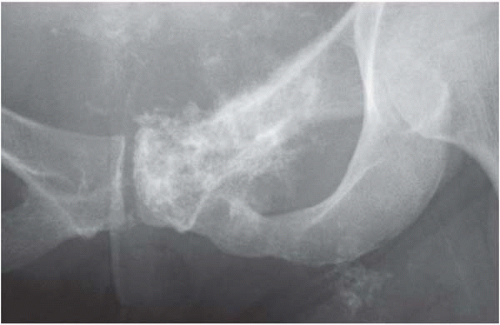
Plain radiograph of the pelvis with a coned-down view of the left superior ramus shows a stippled calcification in the soft tissues adjacent to the left superior pubic ramus (A). There is some calcification with extension into the adductor region of the thigh. Close-up radiograph of the pelvic floor shows stippled calcification and destruction of the left superior pubic ramus, suggesting that the pubic ramus is the primary origin of the tumor (B). This type of calcification is typical of cartilage-forming tumors. The pelvis is the most common site of primary chondrosarcomas. The hip and remaining ilium are unaffected.
CT Scan Report
CT scan of the pelvis shows an extremely large mass involving the true pelvis, extending from the left superior pubic ramus to the left pelvic wall and acetabulum. It then extends across to the right acetabulum, although there is no direct visualized destruction to either acetabuli. This mass shows a marked increase in stippling (calcification) in the inferior portion of the lesion, although the predominant component of the mass shows no matrix formation. The bladder is displaced medially and is compressed. The uterus is displaced anteriorly to the left. The rectum is markedly displaced anteriorly and to the left. Chondrosarcomas of the pelvis typically have an
extremely large soft tissue (extraosseous) component. The “water” density of the tumor suggests a myxoid type of chondrosarcoma. Note the tumor density is similar to that of the bladder. Axial CT below the true pelvis shows tumor and calcification extending into the left adductor region as well as the ischiorectal space. Pelvic chondrosarcomas that extend into the ischiorectal space often involve the urethra and bladder neck. The surgeon must be prepared to resect these structures.
extremely large soft tissue (extraosseous) component. The “water” density of the tumor suggests a myxoid type of chondrosarcoma. Note the tumor density is similar to that of the bladder. Axial CT below the true pelvis shows tumor and calcification extending into the left adductor region as well as the ischiorectal space. Pelvic chondrosarcomas that extend into the ischiorectal space often involve the urethra and bladder neck. The surgeon must be prepared to resect these structures.
▪ MRI
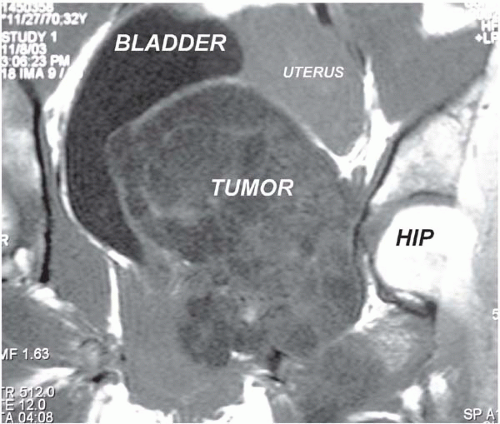 Figure 63.3 |
MRI Report
The T1 coronal view shows an extremely large mass arising from the left superior pubic ramus with large intrapelvic and extrapelvic components and extending well above the level of the iliac crests, involving both the left and right acetabular walls with extension into the left adductor muscle group and destruction of the left superior pubic ramus. The tumor extends across the midline, displacing the bladder and uterus, and lies against the left inner wall of the acetabulum with extension into the ischiorectal space. This mass demonstrates heterogeneosity with some areas of matrix formation. T2 coronal MRI (not shown) reveals obvious extension of the extraosseous component of the tumor arising from the superior pubic ramus. This mass fills the pelvis and extends above the iliac crests. There is obvious extension into the adductor compartment below the left superior pubic ramus.
Differential Diagnosis
The differential diagnosis of a primary tumor of the superior pubic ramus that fills the entire pelvis and has extension into the adductor group muscle is suspicious for a bone sarcoma in this middle-aged patient. This tumor is most likely a chondrosarcoma or one of its variants, although the differential includes metastatic carcinoma (unlikely, because most metastatic carcinomas are not accompanied by large extraosseous components) and osteosarcoma (usually found in adolescents). The other primary bone tumors do not demonstrate such an extensive extraosseous component. Lymphomas of bone may demonstrate extraosseous involvement; however, the CT scan and MRI show matrix (calcification) formation, which is characteristic of a cartilage tumor. Most chondrosarcomas of the pelvis are extremely
large and present with very few symptoms related to the compression of the pelvic contents. The patient’s presenting complaint of pain is nonspecific, and left-sided sciatica is most likely related to compression of portions of the lumbosacral plexus on the left side due to the large tumor mass. Despite the large size of the tumor, this patient had no complaints of urinary or rectal incontinence.
large and present with very few symptoms related to the compression of the pelvic contents. The patient’s presenting complaint of pain is nonspecific, and left-sided sciatica is most likely related to compression of portions of the lumbosacral plexus on the left side due to the large tumor mass. Despite the large size of the tumor, this patient had no complaints of urinary or rectal incontinence.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


