Case 6
Presentation
A 69-year-old woman became aware of a right upper neck swelling during an upper respiratory tract infection. Although the acute symptoms resolved, the mass persisted. She has a history of essential hypertension but is otherwise in very good health. She has smoked 20 cigarettes per day for more than 20 years, but had ceased in the 3 months prior to her presentation. She rarely drinks alcohol. She denies any throat pain, dysphagia, bleeding, or weight loss and has noticed no recent voice change. No skin tumors were removed in the past. Physical examination reveals a mass at least 3 cm in diameter, deep to the anterior border of the sternomastoid muscle with no additional evidence of adenopathy. Inspection of the oral cavity and oropharynx and flexible nasopharyngoscopy reveal no obvious abnormality.
Differential Diagnosis
A lateral neck mass presenting in an older patient, particularly one who smokes, should be considered metastatic carcinoma in a cervical lymph node until proven otherwise. The most likely diagnosis is metastatic squamous cell carcinoma (SCC), either from a mucosal or cutaneous site. Other metastatic tumors would include poorly differentiated or undifferentiated carcinomas, adenocarcinoma from head and neck or infraclavicular primaries, thyroid carcinoma, and melanoma or other cutaneous malignancies. Less commonly, a lateral neck mass may be a primary tumor of the salivary gland or thyroid, or a primary lymphoid tumor. A pulsatile mass may suggest a vascular tumor, such as a carotid body tumor. Rarely, this may be the presentation of a primary or metastatic bone or soft tissue sarcoma.
▪ CT Scans
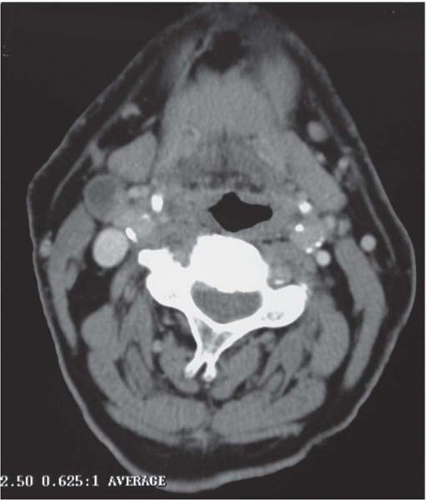 Figure 6.1 |
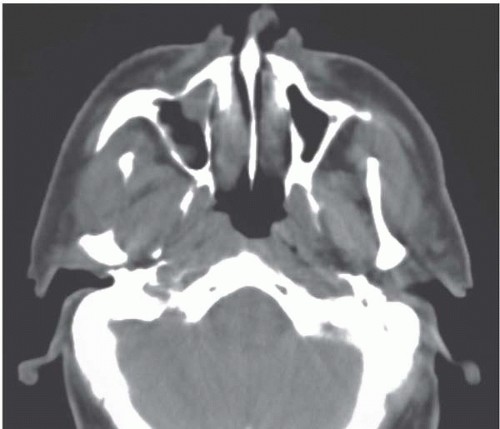 Figure 6.2 |
CT Scan Report
Computed tomography (CT) demonstrates a heterogeneous mass in the upper jugular chain consistent with malignant adenopathy. Figure 6.1 shows a partially cystic lymph node in the upper right neck, and Figure 6.2 reveals subtle asymmetry in the nasopharynx, suggesting a possible primary site.
Case Continued
Ultrasound results confirm the CT findings. Chest radiography reveals no pulmonary lesion. Fine-needle aspiration (FNA) biopsy shows large degenerate or necrotic cells with features consistent with SCC.
Recommendation
The patient is advised to have examination under anesthesia (EUA) and positron emission tomography (PET) scanning as part of an investigational protocol.
▪ Approach
The entire upper aerodigestive tract should be systematically examined with the assistance of rigid endoscopes and, where possible, palpated. In the absence of a suspicious ulcer or tumor mass in the office examination, mucosal asymmetry, induration, or friability may offer the only clues to the presence of a primary tumor. In view of the CT findings, close attention should be paid to the right nasopharynx in this patient. The base of tongue, tonsils, pyriform sinuses, and postcricoid regions frequently harbor small primaries and should be carefully assessed. Biopsies should be taken from any suspicious areas. In the absence of any other abnormality, tonsillectomy should be performed.
Discussion
FNA biopsy is the most appropriate investigation of the neck mass, providing there is no specific contraindication. A diagnosis can be obtained in more than 90% of patients; therefore, open lymph-node biopsy is usually not necessary and is not recommended. If, however, FNA does not provide a diagnosis, current opinion is that an open biopsy can be performed without compromising the long-term outcome.
A thorough history and physical examination, combined with imaging and examination under anesthesia, will uncover a primary site in approximately 50% of patients presenting with a putative unknown primary. A diagnosis of metastatic SCC is easily made, but for diagnoses other than SCC, special stains of the fine-needle aspirate, or additional blood tests such as thyroglobulin, calcitonin, or prostate-specific antigen levels may provide some clue. A finding of adenocarcinoma would prompt further imaging of the thyroid, breast, and gastrointestinal tract. Poorly differentiated or undifferentiated tumors may also have primary sites above or below the clavicles. For 5% to 8% of patients presenting with a malignant neck mass, no primary site will be found.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


