Case 56
Presentation
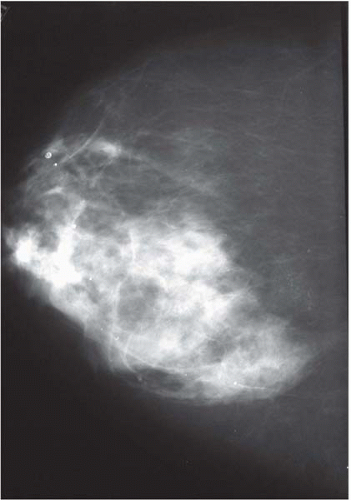
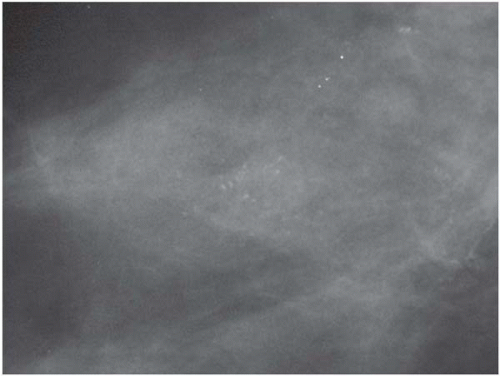
A 45-year-old asymptomatic woman with no significant past medical history undergoes annual screening mammography and presents to your office with an abnormal mammogram report. She has no family history of breast or ovarian cancer. No abnormalities are detected upon physical examination. A review of her current mammogram, with magnification views, demonstrates indeterminate microcalcifications in the upper outer quadrant of the right breast.

Differential Diagnosis
Indeterminate microcalcification may be benign, though the likelihood of malignancy (noninvasive or invasive) needs to be kept in mind. Pathologic diagnosis may include fibrocystic disease, atypical ductal/lobular hyperplasia, lobular carcinoma in situ (LCIS), or ductal carcinoma in situ (DCIS)
Discussion
Calcification can occur both in carcinoma and in adjacent benign breast lesions and may be present in adjacent epitheliosis. The origin and distribution of microcalcification appears to be the same in epithelial hyperplasia, noninvasive carcinoma, and invasive carcinoma, and there may be a relationship between the amount of calcification and the activity of the epithelial cells. Microcalcification is not specific to breast cancer, but is a product of increased cellular activity in the lobuloductal complex and may be extruded into the surrounding interstitial tissue. This implies that microcalcification on the mammogram, particularly if sparse, demonstrates a high-risk area of breast rather than a certainty of the presence of carcinoma.
A retrospective review of 859 cases conducted at the Mayo Clinic analyzed 11 morphologic categories that were encountered in a mammogram and correlated to pathological findings. Within these categories, the percentages of cases with a surgical pathologic diagnosis of malignant involvement were as follows: benign calcification (0% malignant); indeterminate calcification (22%); malignant calcification (92%); smooth mass (1%); irregular mass (40%); architectural distortion (47%); asymmetric breast tissue (3%); smooth mass with calcification (0%); irregular mass with calcification (66%); architectural distortion with calcification (57%); and asymmetric breast tissue with calcification (29%). The overall rate of malignant involvement for the 859 cases was 34%.
Recommendation
Compare with previous mammogram to determine if the microcalcifications are a new finding. If they are a new finding, then stereotactic needle core biopsy (SNCB) should be considered to establish tissue diagnosis. If this procedure is not available, then a needle-localized excisional biopsy should be performed.









