Case 52
Presentation
A 46-year-old woman presents to your office with a large palpable mass in her right breast, which she first noted 7 months earlier. Physical examination reveals thin shiny skin over the central portion of the right breast around the nipple-areolar complex. There is distortion of the nipple-areolar complex. The right breast is larger than the left, and contains a mass measuring 15 × 10 cm, which occupies the entire outer and central portion of the breast. The mass is not fixed to the chest wall and does not invade the skin. There are no palpable right supraclavicular nodes. There is a firm, nonfixed, 1.5-cm node in the right axilla that is clinically suspicious for metastatic disease. Examination of the left breast and axilla is normal.

Differential Diagnosis
The differential diagnosis of a large breast mass such as the one in this case is primarily between breast carcinoma and phyllodes tumor, either benign or malignant.
Discussion
Nonepithelial breast malignancies are rare. A review of 363,801 malignant breast tumors reported to 26 population-based registries between 1994 and 1998 identified only 0.4% (1,401) as nonepithelial in origin. The median age of women with nonepithelial cancer was 53 years, 10 years younger than that of women with epithelial cancer. Clinical characteristics suggestive of adenocarcinoma of the breast rather than phyllodes tumor include skin invasion, ulceration, or peau d’orange. Shiny thin skin is a characteristic of phyllodes tumors, but this is due to pressure necrosis rather than actual skin invasion. On mammography, phyllodes tumors are often smooth or lobulated, with well-defined margins. Ultrasound will occasionally demonstrate fluid-filled, elongated clefts within a solid mass, a classic sign of phyllodes tumors. Although many of these are present in the patient in this case, one aspect of her presentation that was not suggestive of phyllodes tumor was the presence of clinically positive axillary lymph nodes. The malignant component of a phyllodes tumor is sarcomatous, so metastases to axillary nodes are rare. Although clinical and imaging characteristics may suggest phyllodes tumor or epithelial malignancy, a histologic diagnosis is the only method of reliably distinguishing between these entities.
Recommendation
A diagnostic mammogram, ultrasound if necessary, and a core biopsy to establish tissue diagnosis are recommended for this patient.
Case Continued
The mammogram reveals an abnormal large suspicious mass in the right breast. By ultrasound, the mass measured 8.8 cm in diameter and was hypoechoic with heterogeneous internal echoes. A core needle biopsy revealed grade III infiltrating ductal carcinoma with negative hormone receptors and no overexpression of HER-2.
▪ Mammogram
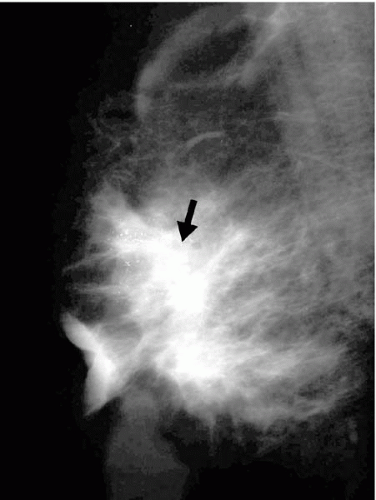 Figure 52.2 |
Mammography Report
On pretherapy mammogram, a large mass occupying the entire lower half of the breast is present. The mass was bilobulated with a poorly defined posterior border.
Diagnosis and Recommendation






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


