Case 51
Presentation
A 45-year-old woman with no significant past medical history was found to have an abnormality in the right breast on routine bilateral screening mammogram. She presents to your office for evaluation and further treatment recommendations. The patient is without any complaints, including nipple discharge, skin changes, tenderness, or palpable mass. There is a family history of breast carcinoma in her paternal aunt at age 70. The patient’s age of menarche was 12 years. Her last menstrual cycle was 2 weeks prior to presentation. The patient is gravida 2, para 1, abortion 1, with her first childbirth at age 35. She has been on birth control pills in the past but currently takes no hormones. On examination, the skin, nipples, and areolas appear normal. There is no skin dimpling with movement of the pectoralis. There is no nipple retraction. No nipple discharge can be elicited. There are no dominant masses in either breast. The axillary tails are normal. The supraclavicular, axillary, and cervical regions are free of significant lymphadenopathy bilaterally.
▪ Mammograms
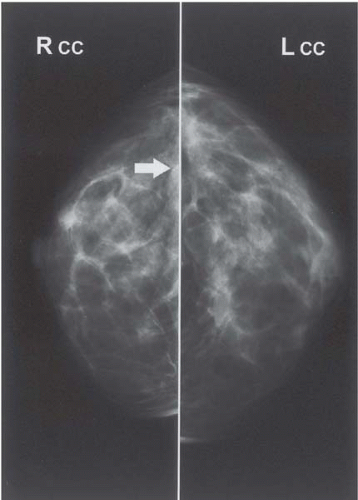 Figure 51.1A |
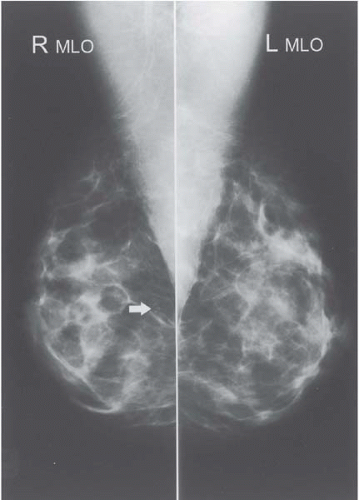 Figure 51.1B |
Mammography Report
On screening mammography of the bilateral breasts in (A) craniocaudal (CC) and (B) mediolateral oblique (MLO) views, white arrows on the right breast mammogram demonstrate fine, linear, heterogeneous calcifications. A new group of clustered fine, linear, heterogeneous, and punctuate calcifications is seen in the lower outer quadrant of the right breast.
Differential Diagnosis
The differential diagnosis for mammographic calcifications includes fibrocystic diseases, true mineral deposits, milk of calcium (calcium within the fluid of a noncancerous cyst), inflammation (mastitis), fibroadenomas, and cancer. In this patient with clustered fine, linear, heterogeneous, and punctuate calcifications, a further diagnostic mammogram of the right breast is needed, including magnified views.
Discussion
Mammography remains the best method of detection for early breast cancer. Calcifications in the breast are common, and most breast calcifications are benign. However, certain patterns or appearances of calcifications can be associated with cancer and further workup is needed to rule out malignancy. There are different types of breast calcifications, such as: microcalcifications, which are very fine calcifications that may be scattered or clustered and can be associated with either benign or malignant lesions; “popcorn” calcifications, which appear fluffy and are benign; macrocalcifications, which are large calcifications that are usually benign; and spiculated calcifications, which appear as spider webs and are associated with cancer.
Recommendation
Additional diagnostic views of the breast are needed to differentiate the microcalcifications in mammography. Magnified views best delineate the shape and extent of calcifications. If calcifications are suspicious (i.e., clustered, pleomorphic, or branched), then biopsy is required to rule out malignancy.
▪ Mammograms
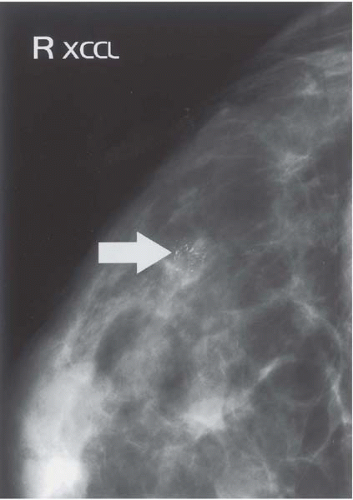 Figure 51.2A |
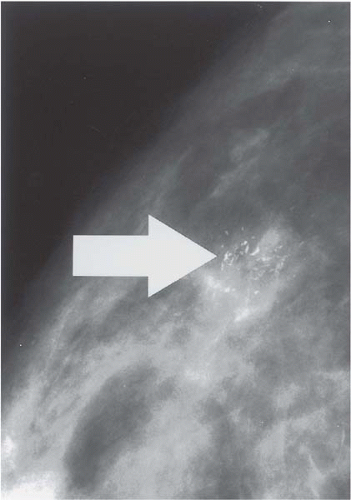 Figure 51.2B |
Mammography Report
Additional diagnostic views of the right breast demonstrate 15 × 20-mm clustered fine linear branching and pleomorphic calcifications in the right lower outer quadrant (white arrows)—(A) exacerated craniocaudal lateral (XCCL) view, (B) magnified XCCL view. Core biopsy is the procedure of choice for the biopsy of a nonpalpable mammographic abnormality.
▪ Specimen Photograph
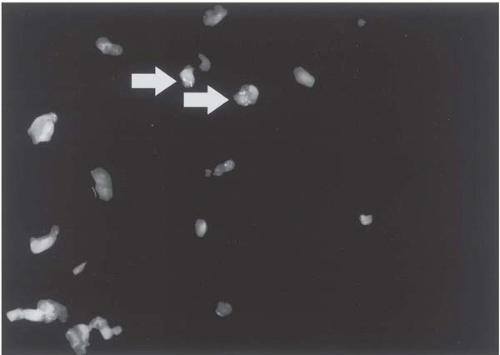 Figure 51.3
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





