Case 42
Presentation
A 72-year-old woman with history of distal gastrectomy for early gastric cancer presents to your office after she was seen by her primary medical doctor with a suspected liver tumor detected by ultrasonography. She received a blood transfusion 30 years ago at the time of gastrectomy. She was diagnosed as having hepatitis C 10 years ago, and has been followed by her primary medical doctor. She denies history of alcohol abuse. On examination, liver and spleen are not palpable and she does not have ascites or jaundice.
▪ Laboratory Tests
Laboratory values on admission were as follows: hepatitis B surface antigen (HBsAg) negative, hepatitis C virus antibody (HCV Ab) positive; platelet count: 8.1 × 104/mm3; prothrombin time: 56.6% (international normalized ratio [INR] 1.48); serum total bilirubin: 1.0 mg/dL; alpha-fetoprotein (AFP): 240 ng/mL (normal range, <9); des-gamma-carboxy prothrombin (DCP): 100 mAU/mL (normal range, <40); 15-minute retention rate of indocyanine green (ICG): 24%; and plasma disappearance rate of ICG: 0.095 (min−1).
Differential Diagnosis
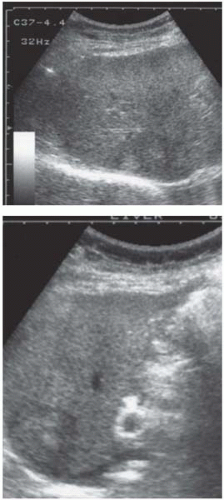
The differential diagnoses for a hypoechoic hepatic mass in the liver are hepatocellular carcinoma, cholangiocellular carcinoma, metastatic liver cancer, and cavernous hemangioma.
Discussion
Development of a liver mass in a hepatitis C-positive patient is usually highly suspicious for hepatocellular carcinoma. Ultrasound (US) findings and elevated serum levels of AFP and DCP are supportive of the diagnosis. Intrahepatic cholangiocellular carcinoma or a mixed type of hepatocellular-cholangiocellular carcinoma are relatively rare but cannot be excluded by US alone. To exclude metastatic liver tumor, common primary sites including the gastrointestinal tract (upper gastrointestinal study, colonoscopy), pancreas, breast, and genitourinary organs should be screened. Liver metastasis from early gastric cancer resected 30 years before is highly unlikely. A cavernous hemangioma is sometimes hypoechoic, but may be ruled out by computed tomography (CT) scan or angiography.
Laboratory data, including decreased platelet count and serum albumin and prolonged prothrombin time, suggest the presence of liver cirrhosis. To estimate the hepatic functional reserve precisely, ICG test is recommended.
Recommendation
A dynamic CT scan study, as well as hepatic angiography.
▪ CT Scan
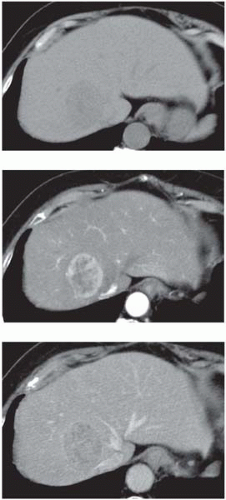 Figure 42.2
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





