Case 4
Presentation
A 55-year-old teacher presents with hoarseness that has worsened over the past month and now interferes with his occupation. He has a history of smoking 10 cigarettes per day for around 20 years. Using the indirect laryngeal mirror and flexible laryngoscope, you detect an irregular 1-cm lesion at the junction of the anterior and middle thirds of the left vocal fold, but mobility is not impaired. The rest of the head and neck examination is normal.
Differential Diagnosis
Because the patient is a smoker, and because dysphonia has persisted for more than 1 month and is worsening, laryngeal carcinoma is the most likely diagnosis, and needs to be confirmed with tissue biopsy. Laryngopharyngeal reflux (LPR) is the most common cause of laryngitis in adults and can present as persistent dysphonia. Features on clinical examination include erythema of the posterior third of the vocal folds and arytenoids, diffuse edema, and granuloma of the vocal process of the arytenoids. Examination of the larynx can reveal a variety of findings: erythema of the posterior third of the vocal folds and arytenoids with interarytenoid mucosal hypertrophy, subglottic edema, or mucosal thickening without significant erythema. Vocal process granulomas, with or without associated laryngeal edema, can be present.
Vocal fold nodules usually result from vocal abuse. They are often bilateral and occur at the junction of the anterior and middle thirds of the true vocal folds.
Laryngeal papillomatosis is caused by human papilloma virus and can present with hoarseness and airway obstruction if the disease is advanced. Characteristically, the laryngeal mucosa is erythematous and edematous, especially over the true vocal folds.
Tuberculous laryngitis is a common granulomatous disease of the larynx. Dysphonia, odynophagia, dyspnea, and odynophonia may occur. It is usually associated with active pulmonary tuberculosis. Laryngeal examination may reveal edematous and hyperemic mucosa involving the posterior third of the larynx or granular exophytic lesions that may mimic carcinoma.
Recommendation
A biopsy is mandatory for confirming the diagnosis. It can be obtained during the panendoscopy, which is necessary to evaluate for synchronous cancer. Computed tomography (CT) scan with contrast enhancement is the method of choice for studying the larynx. CT scan should be performed before biopsy so that abnormalities that may be caused by biopsy are not confused with tumor.
Case Continued
Biopsy reveals a well-differentiated invasive squamous cell carcinoma.
▪ CT Scan
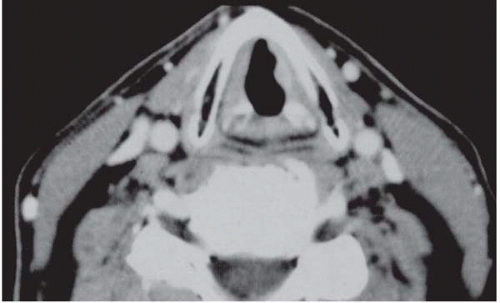 Figure 4.1 |
CT Scan Report
There is tissue thickening with contrast enhancement at the junction of the anterior and middle thirds of the left true vocal fold; there is no infiltration of the paraglottic space or the anterior commissure. The subglottis is not involved. There is no evidence of cartilage invasion or pathologically enlarged cervical lymph nodes.