Case 37
Presentation
A 47-year-old white woman presents with a recent onset of anorectal discomfort and bright red blood per rectum. Digital rectal examination reveals a 1- to 1.5-cm lesion in the rectum, on the anterior aspect just proximal to the anal sphincter.
Differential Diagnosis
The differential diagnosis of a 1.5-cm rectal lesion in this age group commonly includes an adenomatous polyp. The most common malignant cause is a rectal adenocarcinoma (possibly within a tubulovillous adenoma). More rare causes include benign lymphoma, lipoma, leiomyoma, fibroma or hemangioma, and malignancies such as carcinoid, malignant lymphoma, and leiomyosarcoma.
Recommendation
Fresh blood per rectum always requires a full history and thorough clinical examination, including a digital rectal examination, proctoscopy, and flexible sigmoidoscopy in the first instance. The initial management of a rectal polyp is primarily aimed at complete removal of the lesion, obtaining tissue for a histologic diagnosis, and exclusion of other colonic polyps.
Case Continued
The lesion is biopsied for histologic examination, and further investigations are arranged, including colonoscopy and subsequent transanal resection of the lesion. Colonoscopy demonstrates a normal colon beyond this lesion.
▪ Histopathology Slides
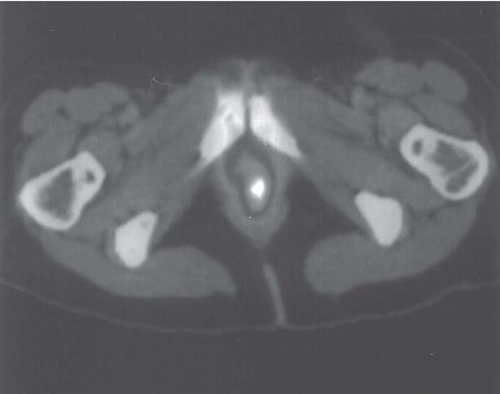 Figure 37.1A |
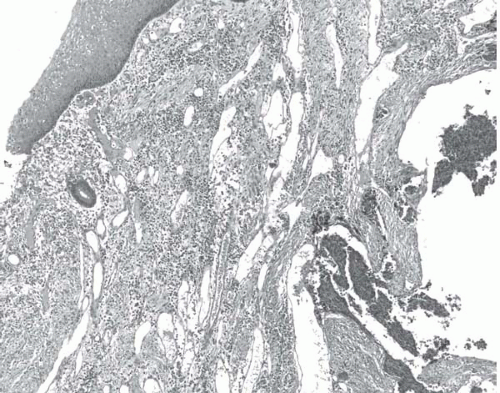 Figure 37.1B |
Histopathology Report
Histology of the removed lesion reveals a deeply invasive (beyond muscularis propria) neuroendocrine tumor or carcinoid, 1.8 cm in diameter, with positive stains for chromogranin A and synaptophysin, moderate atypia, angioinvasion, 1 mitosis in 10 high-power fields (HPF) and a tumor proliferative index (TPI) up to 30%, as assessed by Ki67 immunostaining (World Health Organization [WHO] well-differentiated endocrine carcinoma, or malignant carcinoid). Squamous epithelium at the anorectal margin can be visualized in relation to the distal edge of the resected tumor.
▪ PET Scans
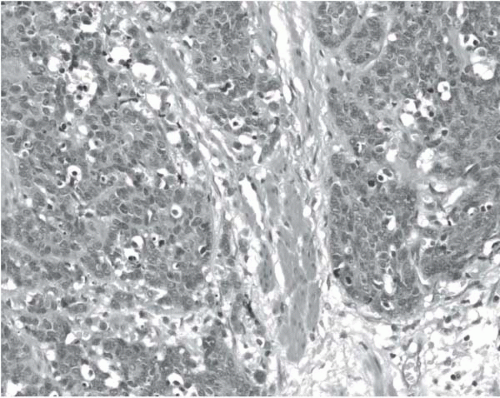 Figure 37.2A |
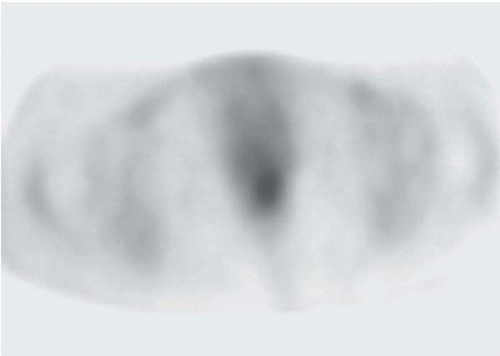 Figure 37.2B |
PET Scan Report
Neuroendocrine tumor is seen extending beyond the muscularis propria. The lesion is located very close to the anorectal junction. The deep resection margin is positive, indicating incomplete removal.
Discussion
The endoscopic features of rectal neuroendocrine tumors are well described, and these findings should be detailed and carefully reported. Central mucosal depression or ulceration suggests high metastatic potential.
Rectal carcinoid tumors are of neuroendocrine origin and, unless particularly poorly differentiated, they contain the typical dense-core secretory granules in the cytoplasm, and small clear vesicles. Synaptophysin is associated with the small vesicles, a sensitive marker for neuroendocrine tumors. Chromogranin A is localized to the secretory granules and is regarded as a powerful universal marker for neuroendocrine tumors.
New classification systems and nomenclature now refer to neuroendocrine tumors (NETs) rather than carcinoids, although this term is still commonly used both in histology reports and the literature. Gastrointestinal NETs may be classified by the site of origin (i.e., foregut, midgut, or hindgut embryologically). The majority of hindgut NETs are found in the rectum.
Three types of neuroendocrine tumors have been identified in the hindgut, L cell tumors, EC cell tumors, and small cell tumors. Rectal tumors are usually L cell tumors, producing glicentin-related products and PP-PYY peptides. The tumors may contain subsets of other neuroendocrine cells among the L cells. Argentaffin EC tumors with typical serotonin production are extremely rare in the rectum.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


