Case 35
Presentation
A 55-year-old man presents with a 3-year history of intermittent bleeding per rectum. He denies weight loss, nausea, or vomiting. Recently he had noted decreased caliber of stool, increasing episodes of liquid stool, and diminished force of the urinary stream. He had never undergone screening colonoscopy.
The patient’s past medical and surgical history is negative. Family history is positive for breast cancer in the patient’s mother. The patient worked as a jeweler and had a 17-pack-year history of cigarette smoking.
Auscultation of the lungs reveals scattered wheezing. The abdomen is soft without intra-abdominal masses or hepatosplenomegaly. Colonoscopy performed by the referring physician had revealed a narrowed rectosigmoid colon with a malignant-appearing polyp at 15 to 22 cm. Biopsies showed adenoma with high-grade dysplasia but no evidence of carcinoma. Rigid proctoscopy showed an apparent tumor at 10 cm above the dentate line, which extended for a minimum length of 5 cm. There was no evidence of hemorrhoids, anal fissure, or other anorectal pathology. Laboratory examination is remarkable for a carcinoembryonic antigen (CEA) level of 24.3 ng/mL (normal: <5 ng/mL).
Differential Diagnosis
The patient’s history of rectal bleeding, coupled with a recent change in stool caliber and consistency, is strongly suggestive of rectal cancer. The elevated CEA level corroborates this. In addition, the history of recent voiding difficulties suggests the possibility of a locally advanced pelvic tumor. The differential diagnosis also includes colitis of diverse etiologies, arteriovenous malformation, hemorrhoids, and anal fissure. However, no anorectal pathology was identified at proctoscopy. Therefore, the first step after physical examination should be to repeat the colonoscopy and biopsies.
▪ Colonoscopic Image
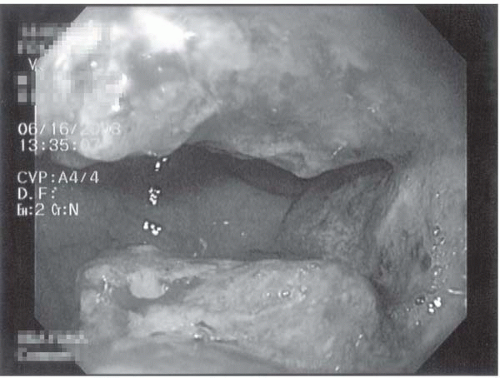 Figure 35.1 |
Colonoscopy Report
Repeat colonoscopy confirmed a malignant-appearing mass, 11 cm above the dentate line.
Pathology Report
Pathologic examination revealed a villoglandular polyp with moderate to severe dysplasia. No definitive evidence of malignancy was seen.
▪ CT Scan
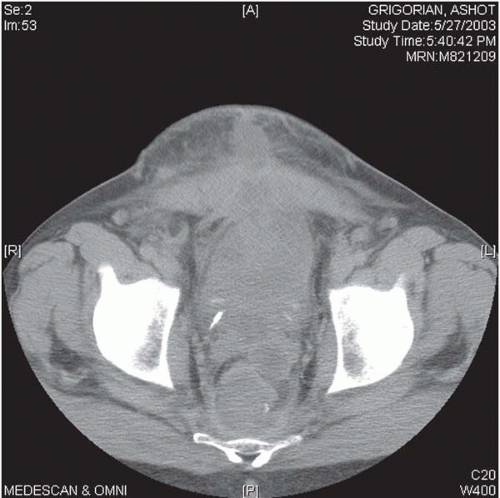 Figure 35.2 |
CT Scan Report
Computed tomography (CT) scan of the abdomen and pelvis with intravenous and oral contrast agents reveals a 7-cm, heterogenous, irregular mass arising from the rectosigmoid junction, adjacent to the prostate. No clear plane is apparent between the tumor and the prostate/base of bladder. No suspicious adenopathy or ascites is seen. A 2.5-cm hypodense mass with peripheral enhancement, consistent with hemangioma, is seen in the dome of the liver. CT scan of the chest shows no evidence of pulmonary metastasis.
Diagnosis
This patient presents with presumed locally advanced rectal cancer, albeit without tissue diagnosis of malignancy.
Recommendation
The goal of surgical management is complete resection of all gross disease. Adhesions to adjacent organs are malignant in up to 80% of cases and should not be divided; instead, en bloc resection with a rim of normal tissue of the involved organ(s) is required. Neoadjuvant chemoradiation followed by surgical resection is the optimal treatment for this patient presenting with locally advanced rectal cancer. In addition, the use of neoadjuvant chemoradiation increases the likelihood of performing a successful sphincter-sparing procedure for primary resection (rather than abdominoperineal resection). The addition of intraoperative radiotherapy (IORT) to chemotherapy and external beam radiation therapy (EBRT) may significantly improve local control and provide further survival advantage over neoadjuvant chemoradiation followed by surgical resection; however, IORT is available only at select centers.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


