Case 32
Presentation
You are called to the emergency department to evaluate a 44-year-old white man who presents with a 2-month history of intermittent lower abdominal pain, which became acutely worse over the last 24 hours with associated abdominal distention. He also had nausea and vomiting with absence of bowel movements for at least 1 week. He is passing flatus, but much less than normal. He describes a change in bowel habit as constipation intermixed with diarrhea for the last 2 months, and he had an episode with hematochezia. He describes a 10-lb weight loss with a fair appetite. Upon examination, the patient appears pale and in some discomfort, but there is no evidence of jaundice. His abdomen is distended with tenderness in the right lower quadrant, but no guarding or rigidity. Bowel sounds are high pitched and hyperactive. Rectal examination reveals no masses.
Differential Diagnosis
The clinical presentation is suggestive of acute on chronic large bowel obstruction. When faced with suspected bowel obstruction, the surgeon needs to address three specific issues:
Is this obstruction simple or strangulated? Physical examination in conjunction with basic laboratory tests is indispensable in determining whether there is any evidence of jeopardy to the blood supply to the involved bowel. The presence of localized guarding, rigidity, and absent bowel sounds associated with elevated white blood cell (WBC) count and elevated amylase and lactate acid levels is indicative of compromised bowel. In this case, the tenderness in the right lower quadrant is concerning, and it may be due to a grossly distended or compromised cecal wall resulting perhaps from a distal large bowel obstruction.
What is the level of obstruction? The level of obstruction can often be ascertained from plain radiographs of the abdomen taken in the supine and erect positions. A Gastrografin enema or, even better, a computed tomography (CT) scan of the abdomen and pelvis in a stable patient can provide valuable information regarding the cause of intestinal obstruction.
What is the cause for the obstruction? In an adult, the etiology of obstruction is usually obvious from the clinical history and physical examination. Important causes include external hernia, adhesions from previous abdominal surgery, carcinoma of the colon, diverticular stricture, and volvulus. Given the history of change of bowel habit with hematochezia and weight loss, the diagnosis of left-sided colon carcinoma should be strongly considered.
Recommendation
Obtain complete blood cell count (CBC), Chem 7 (tests for glucose, blood urea nitrogen, creatinine, potassium, sodium, chloride, and carbon dioxide), amylase level, lactic acid level, and radiograph of the abdomen in supine and erect positions. Initiate fluid resuscitation and decompression of the bowel with nasogastric tube.
Case Continued
Intravenous fluid consisting of lactated Ringer’s solution is commenced, and nasogastric tubing and Foley catheter are placed. His laboratory tests reveal the following: WBC count 14,000, hemoglobin 10,
hematocrit 33, and serum amylase and lactic acid levels are normal. After physical examination, 4 mg of morphine is administered intravenously for pain control.
hematocrit 33, and serum amylase and lactic acid levels are normal. After physical examination, 4 mg of morphine is administered intravenously for pain control.
▪ Abdominal X-Ray
 Figure 32.1 |
Abdominal X-Ray Report
There are dilated loops of small bowel as well as a grossly distended large bowel, which appears to abruptly end near the descending colon. There is no air in the rectum. The cecum is dilated and measures 7 cm at its widest dimension.
Recommendation
The clinical presentation and plain radiographs are highly suggestive of an obstruction in the left colon. Because there is no clinical evidence of acutely compromised bowel and no peritonitis, a CT scan of the abdomen and pelvis may be valuable.
▪ CT Scan
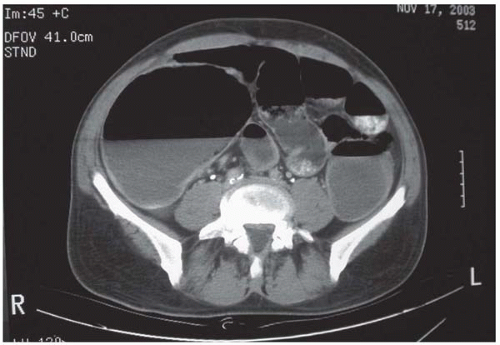 Figure 32.2A |
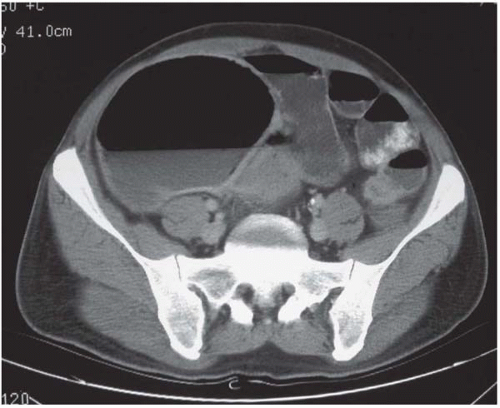 Figure 32.2B |
 Figure 32.2C |
CT Scan Report
An 8-cm complex liver lesion is seen in the left lateral lobe, which is highly suggestive of a metastatic lesion. The dilated small and large bowels are seen, with a 3-cm area of thickening and associated narrowing in the sigmoid colon. There is no evidence of suspicious periaortic lymphadenopathy.
▪ Approach
The clinical presentation and the findings on imaging studies strongly suggest the presence of a colon carcinoma presenting as acute large bowel obstruction with a synchronous liver metastasis. A serum sample should be sent to establish a preoperative carcinoembryonic antigen (CEA) level, which, if elevated, would be useful for comparison during postoperative follow-up.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


