Case 30
Presentation
A 62-year-old man presents with a recent episode of bright red blood per rectum. He denies any weight loss, anemia, obstructive symptoms, or change in bowel habits. There is no family history of colon carcinoma. The abdomen is soft with no apparent masses. Digital rectal examination reveals no palpable lesion. The patient undergoes a colonoscopy.
▪ Colonoscopic Images
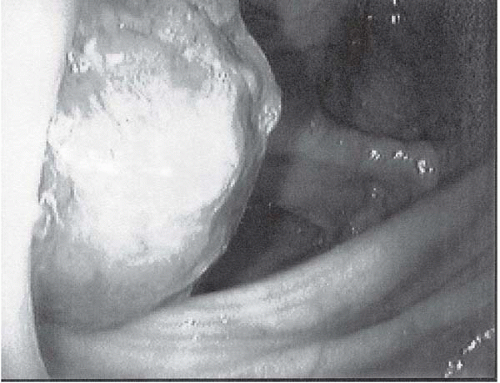 Figure 30.1 |
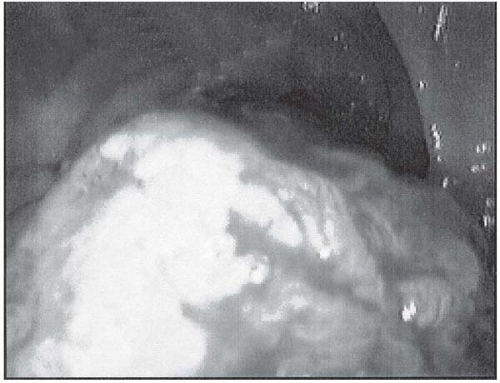 Figure 30.2 |
Colonoscopy Report
A sessile multilobulated 4-cm polyp is found in the ascending colon. The polyp is not amenable to complete polypectomy; therefore, piecemeal polypectomy is attempted. The site of the polyp is marked with 1 mL of India ink; no other polypoid lesions are identified.
Pathology Report
Tubulovillous adenoma with foci of moderately differentiated adenocarcinoma.
Differential Diagnosis
The differential diagnosis for early colon carcinoma is adenomatous polyps of the colon. The risk of adenocarcinoma arising in these polyps is relative to the size of the polyp. A sessile lesion has a greater risk of malignancy than a pedunculated polyp. In this patient, with a large sessile polyp, adenocarcinoma in an adenomatous polyp is highly probable.
Discussion
Colonoscopy is regarded as the most effective screening modality for the detection of early colon carcinoma. It enables a visualized surveillance of the entire colon as well as biopsy or removal of grossly abnormal lesions. Synchronous or metachronous carcinoma can also be excluded during this procedure.
It is generally accepted that the majority of colorectal cancer tracks an adenoma-carcinoma sequence. An adenoma smaller than 1 cm has an approximately 1% risk of malignancy. Conversely, polyps larger than 2 cm have a 35% to 50% incidence of associated carcinoma. The histologic presentation of adenomatous polyps consists of tubular, tubulovillous, and villous. The malignant potential augments with increased villous glandular formation. The malignant potential also correlates with histologic degree of dysplasia. Polyps with severe dysplasia have about a 50% incidence of malignancy. Other adverse risk factors of malignant polyps are
lymphovascular invasion, poorly differentiated or mucinous adenocarcinoma, tumor budding, a flat or depressed lesion, and depth of tumor invasion into the lower third of the submucosal level, although these characteristics may be difficult to determine.
lymphovascular invasion, poorly differentiated or mucinous adenocarcinoma, tumor budding, a flat or depressed lesion, and depth of tumor invasion into the lower third of the submucosal level, although these characteristics may be difficult to determine.
Sessile polyps have a reportedly higher incidence of lymph node metastasis than pedunculated polyps, ranging from 12% to 25%. Therefore, sessile polyps often require more aggressive surgical treatment for curability than pedunculated polyps.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


