Case 3
Presentation
A 38-year-old man of Southern Chinese ancestry presents to your office with a 3-month history of a progressively enlarging left neck mass associated with intermittent right nasal obstruction. He is otherwise well with no other symptoms. He has no significant past medical or family history and is a nonsmoker.
On physical examination, the only significant finding is an enlarged, firm left upper cervical lymph node measuring 4 × 3 cm in diameter. Cranial nerve examination is normal and no abnormalities are found in other systems.
You perform a flexible nasal endoscopic examination of the nasopharynx.
▪ Endoscopic Image
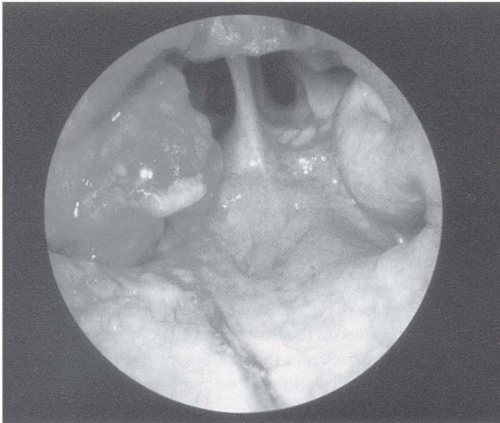 Figure 3.1 |
Endoscopy Report
There is a soft-tissue mass involving the left lateral and posterior walls of the nasopharynx.
Differential Diagnosis
The differential diagnosis for nasopharyngeal masses in the adult includes primary nasopharyngeal carcinoma (NPC), non-Hodgkin’s lymphoma (e.g., natural killer-cell lymphoma), rhabdomyosarcoma, plasmacytoma, and adenocarcinomas of minor salivary glands. The undifferentiated and nonkeratinizing histological subtypes of NPC (World Health Organization [WHO] classification, 1991 edition, WHO types II and III) are most commonly found in Southeast Asian patients (e.g., Southern China, Hong Kong, Taiwan), whereas the keratinizing subtype (WHO type I) is more commonly found in North American or white populations. In this patient of Chinese ancestry with nasal obstruction, undifferentiated NPC is the most likely diagnosis.
Case Continued
Histopathological examination of an endoscopic biopsy of the nasopharyngeal tumor shows an undifferentiated nasopharyngeal carcinoma with strong nuclear staining for Epstein-Barr virus (EBV)-encoded RNA (EBER).
EBER is an important histological marker for NPC because it can be found in most NPC cells, with a preponderance for tumors of the undifferentiated subtype.
Discussion
NPC is endemic in Southern China, North Africa, parts of the Mediterranean basin, and the far Northern Hemisphere (e.g., Alaska, Greenland), where the disease is linked to genetic and dietary factors and is etiologically associated with EBV. The prevalence is highest in Southern China, where as many as 80 (range 10 to 150) cases per 100,000 population are reported each year. The prevalence is lowest in North America, western Europe, and Japan (one case per 100,000 population per year), where the disease is linked to tobacco and alcohol use.
The most common presenting symptom is painless cervical lymphadenopathy. Tumors limited to the nasopharynx may result in nasal symptoms such as epistaxis or obstruction. As the tumor invades the nearby soft tissues, symptoms such as tinnitus, deafness, and recurrent otitis media resulting from eustachian tube obstruction may occur. Advanced tumors invading the base of the skull or the infratemporal fossa may lead to headaches or multiple cranial nerve palsies. Histological confirmation is made primarily via biopsy of the nasopharynx with a fiberoptic nasopharyngoscope. The primary tumor should be evaluated via both computed tomography (CT) and magnetic resonance imaging (MRI) of the nasopharynx and the skull base. These scans are preferably performed before tumor biopsy, because biopsy may cause soft-tissue swelling or a hematoma, rendering radiological interpretation difficult. MRI is more sensitive than CT in evaluating the extent of soft-tissue and neurovascular invasion by the primary tumor, as well as the presence of regional nodal metastasis (especially in the retropharyngeal group of lymph nodes). However, CT is a better tool for defining bone erosion. Nonetheless, both CT and MRI are not sensitive tools for distinguishing locally recurrent or residual disease following radical radiotherapy. There is emerging evidence that positron emission tomography (PET) has a sensitivity of 100% and a specificity of 93% to 96% for detecting recurrent or residual disease at the nasopharynx, compared to 72% and 88% for CT.
Case Continued
As part of the disease staging, MRI and CT scans of the nasopharynx and neck are obtained.
▪ MRI
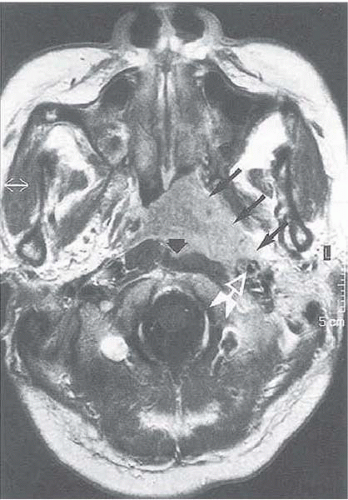 Figure 3.2 |
MRI Report
A T1-weighted, contrast-enhanced image of the nasopharynx reveals a nasopharyngeal soft-tissue mass involving the left lateral wall, the posterior wall, and the roof of the left nasopharynx. The tumor extends into the parapharyngeal space, partially encasing the carotid artery. There is inferior extension of the tumor into the oropharynx along the left lateral wall. The anterior nasal space is not involved. There is no involvement of the skull base. Enlargement of the left deep cervical chain is noted (5 × 4 cm maximum diameter). Retropharyngeal and supraclavicular nodes are not enlarged. Black arrows indicate the location of the primary tumor.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


