Case 27
Presentation
An 11-year-old girl presents with acute appendicitis. An emergency appendectomy is performed, and an acutely inflamed, thickened, and perforated appendix is found. Macroscopic examination of the inflamed appendix reveals a solid tumor obstructing the proximal lumen with a maximum diameter of 14 mm.
Differential Diagnosis
The incidental finding of a tumor in an acutely inflamed appendix at histologic examination is a well-recognized presentation of an appendiceal carcinoid tumor. Carcinoid is regarded as the most common tumor of the appendix, though highly unusual in this age group. Postmortem studies have demonstrated a high incidence of appendiceal carcinoid (up to 1%) tumors that are not clinically apparent.
The pathologist should differentiate between benign and malignant carcinoid tumors. Benign carcinoids are no longer included in cancer registries. When considering primary malignancies of the appendix in all age groups (excluding benign carcinoids), mucinous adenocarcinomas are the most common (37%), followed by colonic-type adenocarcinomas (25%), malignant carcinoid tumors (20%), goblet cell carcinoids (adenocarcinoids; 14%), and rarely signet ring cell carcinomas (4%) (Surveillance, Epidemiology, and End-Results [SEER] Program data, 1973-1998).
Malignant carcinoids occur at a mean age of 38 years, and goblet cell carcinoids at 52 years, whereas adenocarcinomas occur at 60 years of age or later. Histologic examination of the removed appendix is performed.
▪ Histopathology Slides
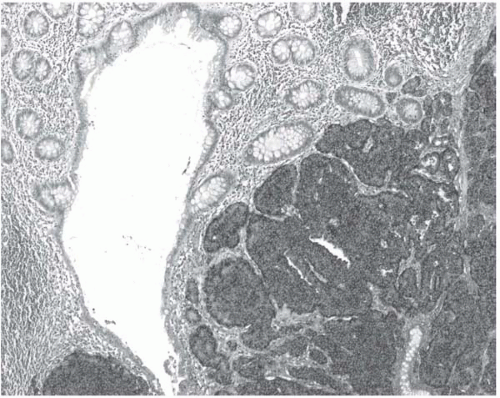 Figure 27.1 |
Histopathology Report
The morphological appearances on histology are those of a malignant carcinoid tumor. Immunohistochemistry confirms the diagnosis, with strong staining with chromogranin A (Fig. 27.1), synaptophysin, and serotonin. The tumor extends through the muscularis and serosa out to the surrounding fat and is present on the serosal surface. A distinct mesoappendix could not be identified, and it is not clear if the fatty infiltration constitutes mesoappendiceal involvement. The proximal resection margin is clear. No vascular invasion is identified.
Very few mitoses are seen, and the cycling rate using Ki67/MIB-1 is less than 3%. Ki67 staining demonstrates the low cycling index of the tumor cells and the higher proliferation index of the normal mucosal cells.
Diagnosis
A 14-mm appendiceal neuroendocrine tumor with carcinoid features.
Discussion
Carcinoid tumors are neuroendocrine tumors originating from endodermal neuroendocrine cells. These cells originate from the same progeny cells as other gastrointestinal cells and are endogenous to the gut, producing important gut hormones such as serotonin and gastrin.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


