Case 22
Presentation
A 46-year-old woman with no significant medical history visits her primary physician with vague epigastric pain. She is noted to have a large mass in the upper abdomen and is referred to your office. She is a nonsmoker and drinks no alcohol. There is no family history of cancer. On examination, she appears slightly anemic, and a mobile, 1-cm upper abdominal mass is palpable. On rectal examination, the mass is not palpable and there is no clinical evidence of ascites. Upper gastrointestinal imaging (UGI) series and endoscopy are ordered.
▪ Clinical Photograph
 Figure 22.1 |
Physical Examination Report
A large mass is localized to the upper right abdomen.
▪ UGI Series and Endoscopy
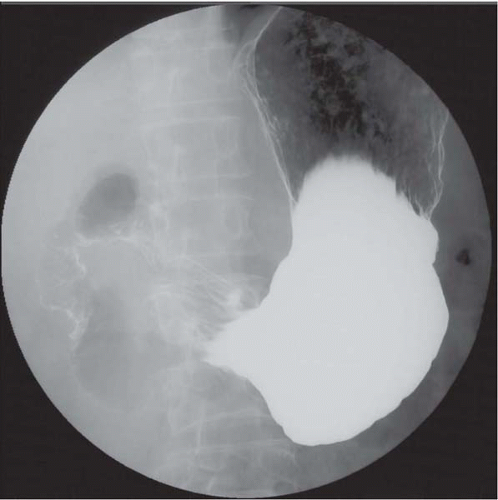 Figure 22.2A |
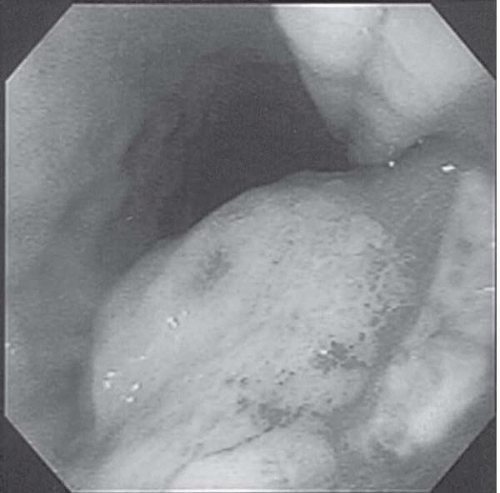 Figure 22.2B |
UGI Series and Endoscopy Report
The esophagus is normal. In the stomach, the greater curvature appears to be compressed by a large tumor. There are bridging folds found by the UGI series and no tumor ulcer is found by endoscopic examination. Endoscopic biopsy reveals normal epithelial cells and no malignant cells.
Differential Diagnosis
The differential diagnosis for submucosal tumors (SMTs) in the adult stomach includes (a) mesenchymal tumors; (b) lymphomas (mostly mucosa-associated lymphoid tissue [MALT] lymphomas, such as high-grade MALT and low-grade MALT); (c) epithelial malignancies, such as stomach carcinoma and gastric carcinoid; (d) congenital diseases; (e) inflammation or inflammatory tumors, such as inflammatory fibroid polyp; and (f) extragastric tumors that compress the stomach.
SMTs frequently show bridging folds and a center spot ulcer in the UGI series and endoscopic examinations.
Discussion
Mesenchymal tumors include stromal cell tumors such as gastrointestinal stromal tumors (GISTs), myogenic tumors (leiomyoma or leiomyosarcoma), and neurogenic tumors (mostly schwannomas in the stomach), lipomas, hemangiomas, lymphangiomas, and granular cell tumors. Mesenchymal tumors sometimes form central ulceration, and biopsies of these areas are often nondiagnostic. Lymphomas and carcinomas mimicking SMT-like tumors sometimes demonstrate slight mucosal changes. Most carcinoma-forming SMT-like tumors are poorly differentiated carcinomas. Congenital diseases include aberrant pancreas and gastric duplication, in which ductal components or cystic lesions are sometimes found in the submucosal area. Aberrant pancreas is most frequently found in the lower third, but may also be located in the body, of the stomach. Gastric submucosal tumors are frequently asymptomatic until they become large. When symptomatic, most patients suffer from hematemesis and/or melena, iron-deficiency anemia, a palpable abdominal mass, and dull abdominal pain. Gastric SMTs form three types of growth: intraluminal, extragastric, and combined. Large tumors tend to form extragastric or combined growth.
The most frequent gastric mesenchymal tumors (70% to 80%) forming submucosal tumors are GISTs; the rest are myogenic tumors (leiomyoma or leiomyosarcoma) and schwannomas. GISTs are preferentially located in the upper and middle stomach, myogenic tumors in the upper third of the stomach around the gastroesophageal junction, and neurogenic tumors along the lesser curvature. GISTs demonstrate the most aggressive behavior compared to the other two mesenchymal tumors. These three stromal tumors in the gastrointestinal tract, however, show very similar macroscopic appearances and they cannot be discriminated from each other by conventional radiographic or endoscopic examinations. They can be differentiated primarily by pathologic examination.
Recommendation
A computed tomography (CT) scan of the abdomen and endoscopic ultrasound as well as endoscopic ultrasound-guided aspiration biopsy. Transcutaneous needle biopsy is not recommended because of the risk of peritoneal seeding.
Case Continued
The patient has a CT scan of the abdomen and pelvis. An endoscopic sonography and endoscopic ultrasound-guided aspiration biopsy are performed.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


