Case 21
Presentation
A 63-year-old man with no significant past medical history is sent from his family physician for evaluation of his epigastric abdominal pain, early satiety, and a 20-pound unintentional weight loss over a 2-month period.
Differential Diagnosis
The differential diagnosis for epigastric pain includes gastritis, gastroparesis, gastroesophageal reflux disease, gastric carcinoma, peptic ulcer disease, Ménétrier’s disease, pancreatitis, pancreatic cancer, biliary colic or acute cholecystitis, colon cancer, and inflammatory bowel disease. Given his age, the duration of symptoms, and particularly the history of weight loss, a neoplastic process should be at the top of the differential.
Case Continued
He has no history of ulcer disease and denies tobacco or alcohol use or blood in his stools. His last colonoscopy, performed 18 months ago, was normal. On physical examination, his scleras are anicteric and there is no supraclavicular adenopathy. There is a firm mass occupying the entire left upper quadrant extending across the midline, and the liver is palpable 7 cm below the costal margin. A computed tomography (CT) scan of the abdomen is ordered.
▪ CT Scan
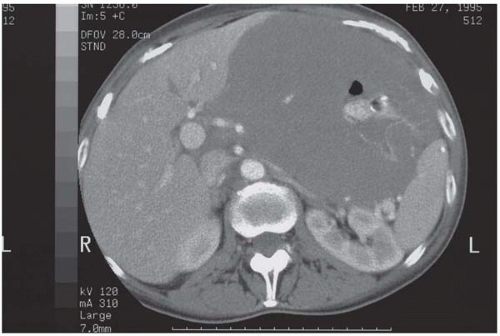 Figure 21.1 |
CT Scan Report
Extensive thickening and irregularity of the gastric wall with minimal contrast in the lumen and displacement of the left lateral segment of the liver to the right of the midline.
Case Continued
Given the CT scan findings, an endoscopy is performed, which revealed an ulcerated mass. Biopsies from the margins demonstrate sheets of large atypical lymphoid cells infiltrating the lamina propria and submucosa. The cells stain CD20 positive and CD3 negative, and the morphology is consistent with diffuse large B-cell lymphoma.
Diagnosis
Primary intermediate-grade B-cell gastric lymphoma.
Recommendations
Treatment with chemotherapy with or without radiation is recommended, reserving surgery for the complications of the chemotherapy, recurrences, or failure of the primary therapy to achieve a complete response.
Discussion
Historically, any discussion regarding the management of gastric lymphoma has included chemotherapy, radiation, and surgery, either in combination or alone. Recently, however, with improved understanding of the pathophysiology of gastric lymphoma, as well as treatment responses and survival, there has been a shift to treating this disease initially with chemotherapy with or without radiation and reserving surgery for the complications of the chemotherapy, recurrences, or failure of the primary therapy to achieve a complete response. Even in the latter two instances, second-line chemotherapy remains effective and is therefore an option along with surgery.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


