Case 16
Presentation
A 76-year-old man complains of progressive dysphagia for 2 months. He can tolerate only a liquid diet. The hold-up sensation is at the level of the throat; he also frequently regurgitates the fluid that he drinks. He has lost 20 pounds during the same time, and his voice has been hoarse for the past week. He used to be a heavy smoker, but gave up smoking 5 years ago. Physical examination shows a thin man with no cervical lymphadenopathy.
Differential Diagnosis
In an elderly man with symptoms of progressive dysphagia and weight loss, an obstructive malignant growth has to be considered in the upper aerodigestive tract. Cancer of the esophagus is probable; extrinsic compression from cancer of the lung or its associated involved lymph nodes in the mediastinum is also part of the differential diagnosis. Other tumors are less common. A cancer of the larynx with obstruction to the esophagus is a possibility, but hoarseness usually predates the dysphagia. More likely, the hoarseness of voice is related to involvement of the recurrent laryngeal nerve. The level of the complaint of dysphagia does not necessarily equate to the level of the physical obstruction. The hold-up sensation is usually located above, but not below, the actual site of cancer.
Recommendation
A barium contrast swallow and an endoscopy are arranged.
Case Continued
The patient aspirates a small amount of barium with the first swallow, and therefore the procedure is abandoned. On endoscopy, a tumor is found extending from the postcricoid area to the cervical esophagus. It extends to 19 cm when measured from the incisors. The endoscope is advanced through with some negotiation. The rest of the esophagus is normal, and so are the stomach and the second part of the duodenum. Because the patient experiences significant obstruction and has lost a substantial amount of weight, a guide wire is passed and a finebore feeding tube is fed down to the stomach for nasogastric tube feeding. At the same setting, a bronchoscopy is also performed to examine the tracheobronchial tree. Right vocal cord paralysis is noted. There is no lesion found inside the airway. Biopsies are taken from the tumor, which proves to be a squamous cell cancer.
Discussion
The diagnosis of cervical esophageal cancer is made. The barium aspiration suggests either high proximal tumor obstruction or that the patient has vocal cord paralysis. The vocal cord palsy is related to either involvement of the right recurrent laryngeal nerve by metastatic lymph node or primary tumor infiltration of the tracheoesophageal groove. It is mandatory to perform a panendoscopy of the upper aerodigestive tract to (a) detect synchronous or metachronous tumors, which can occur in up to 10% of patients due to the phenomenon of field cancerization, and (b) look for tracheal infiltration by the esophageal cancer. Nasogastric tube feeding helps improve the patient’s nutritional status since substantial weight loss has occurred, and is preferred over parenteral nutrition. It is customary to consider a weight loss of more than 10% of the usual body weight to be significant, and that may be associated with poor outcome.
Diagnosis and Recommendation
Cervical esophageal squamous cell carcinoma. Further staging and diagnostic workup are needed to establish the extent of the disease, which will determine treatment approach.
▪ PET/CT Scan
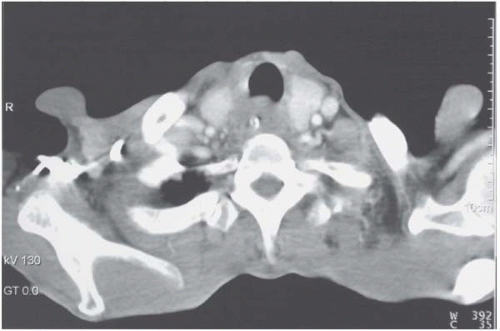 Figure 16.1 |
PET/CT Scan Report
Mural thickening of the cervical esophagus extends from the cricoid cartilage to just above the sternal notch, measuring 8 cm in length. The plane between the right thyroid lobe and esophagus is unclear, suggestive of infiltration. The standard uptake value (SUV) is 9.8. Some small lymph nodes of less than 5 mm are seen in the paraesophageal region, but all have low SUVs of less than 2.0. No distant metastases are detected. The patient has no contraindication to major surgery.
▪ Approach
A diagnosis of locally advanced cervical esophageal cancer is made. Treatment options include chemoradiation or surgical resection with or without adjuvant therapy. For most patients with significant cervical esophageal involvement, surgical resection involves a pharyngolaryngoesophagectomy. The lack of head-to-head comparisons of the two approaches and evidence-based data should be clearly discussed with the patient in order to formulate a treatment plan.
Discussion
Chemoradiation is increasingly used as primary treatment because the magnitude of surgical resection is substantial and laryngeal preservation is possible. Depending on tumor stage, when chemoradiation is used with a curative intent, good local control has been reported. The main drawbacks of chemoradiation are (a) substantial esophagitis and systemic and local symptoms during treatment; (b) stricture formation; (c) future salvage surgery may be made more difficult due to prior radiation; and (d) laryngeal dysfunction both during and after radiation can lead to aspiration symptoms. Laryngeal preservation surgery is possible in tumors of the distal cervical esophagus where a margin from the cricoid can be obtained, or when downstaging has been obtained with chemoradiation. Preserving the larynx, however, may lead to inadequate oncologic clearance. It also predisposes to aspiration, because of an anastomosis very close to the cricoid, and pharyngolaryngeal dysfunction, especially when the recurrent laryngeal nerves can be injured at surgery. For patients with hypopharyngeal tumors or proximal cervical esophageal tumors, segmental resection with reconstruction by a free jejunal graft can be
performed. Alternative voice rehabilitation is required, but aspiration is not problematic because the airway and food passage will be permanently separated.
performed. Alternative voice rehabilitation is required, but aspiration is not problematic because the airway and food passage will be permanently separated.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


