Case 15
Presentation
An 18-year-old man, with no significant past medical history, presented with a 19-months’ history of an indolent mass of the anterior right thoracic cage. The mass had slowly increased in size. The neoplasia has a bony consistency, and is fixed to the ribs without signs of cutaneous inflammation.
▪ Chest X-Ray
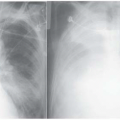
 Figure 15.1 |
Chest X-Ray Report
Opacity of the left anterior thoracic wall with well-defined margins. Osteolysis of the anterior segment of the third left rib.
Differential Diagnosis
The possible diagnoses for this presentation include chondroma, osteochondroma, fibrous dysplasia, desmoid tumor, chondrosarcoma, Ewing’s and Askin’s sarcomas, osteosarcoma, and solitary myeloma. Each of these pathological entities has unique characteristics and specific radiological features that are of diagnostic value.
Chondroma develops during the pediatric years and becomes clinically evident in the age group of 10 to 50 years. These are usually small and asymptomatic, and are usually localized at the costochondral junction. Radiographically, they appear lobulated and radiodense, without cortical bone invasion or soft-tissue swelling.
Osteochondroma (synonym: solitary exostosis) is rare, appears between 10 and 18 years of age, is usually asymptomatic, and grows slowly during skeletal development. Radiologically, the newly formed bone is represented by cancellous bone, irregularly distributed with “finger-like” evaginations.
Fibrous dysplasia usually arises between the ages of 5 and 20 years as an asymptomatic mass in the posterior part of the thoracic cage. There is usually a history of an antecedent traumatic event. Radiographically, these appear as a central fusiform osteolytic area of the rib, with the cortex eroded from inside. The boundaries are clear or slightly faded, without associated calcification.
Desmoid tumor is observed more frequently in females during the third or fourth decade of life. The clinical presentation is of a slowly growing soft-tissue mass, without any particular radiographic appearance, although magnetic resonance imaging (MRI) may be valuable.
Chondrosarcoma is a tumor of the adult age. It can be associated with mild and intermittent pain and progressive growth with invasion into soft tissues. The radiographic picture represents an osteolytic tumor with interruption of the cortex. Calcifications
are evident in the well-differentiated varieties, whereas they are rare or totally absent in the high-degree malignancies (grade 3-4, dedifferentiated). Calcifications are morphologically characterized by irregular granules, nodules, or radiopaque rings. Aggressive varieties are characterized by an interruption of the cortex with invasion of soft tissues by a noncalcified tumor.
are evident in the well-differentiated varieties, whereas they are rare or totally absent in the high-degree malignancies (grade 3-4, dedifferentiated). Calcifications are morphologically characterized by irregular granules, nodules, or radiopaque rings. Aggressive varieties are characterized by an interruption of the cortex with invasion of soft tissues by a noncalcified tumor.
Ewing’s and Askin’s (Primitive Neuroectodermal Tumors) sarcomas are childhood or youth tumors, exceptional before 5 years of age and after 25 years. The first symptom is usually intermittent mild pain that becomes progressively intense, with or without the presence of a mass. Radiologically, these have an onion-peel appearance resulting from periostal bone formation by multiple osteogenetic nuclei infiltrating the medullary spaces and the haversian canals.
Sternal or costal osteosarcoma is rare, presenting between the ages of 10 and 30 years. It manifests with intermittent mild pain. Laboratory studies demonstrate an elevated alkaline phosphatase. The radiograph reveals a tumor growing within the cortical and cancellous bones, which are rapidly destroyed. The periosteum is surpassed, and generally there is a neoplastic production of osteoid and bone tissue.
Myeloma (synonym: plasmacytoma) is observed after 40 to 50 years of age. It is localized in ribs, clavicula, and sternum, with diffuse vague symptoms generally associated to asthenia and fever. Laboratory findings show an elevated plasmacellular percentage, immature and atypical elements, a high percentage of globulins with inversion of the albumin/globulin ratio, and Bence-Jones proteinuria. If solitary, the myeloma presents radiologically as multiple large areas of osteolysis, with or without cortical erosion.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


