Case 12
Presentation
An asymptomatic 65-year-old woman with a 40-pack-year smoking history recently relocated and presents to the office of her new primary care physician. She undergoes an initial physical examination that includes a routine chest radiograph. The chest x-ray raises the question of a faint nodular density in the right lung. The primary physician orders a computed tomographic (CT) scan of the chest and a positron emission tomographic (PET) scan, and sends the patient to a pulmonologist who performs pulmonary function testing and a bronchoscopy.
▪ CT Scan
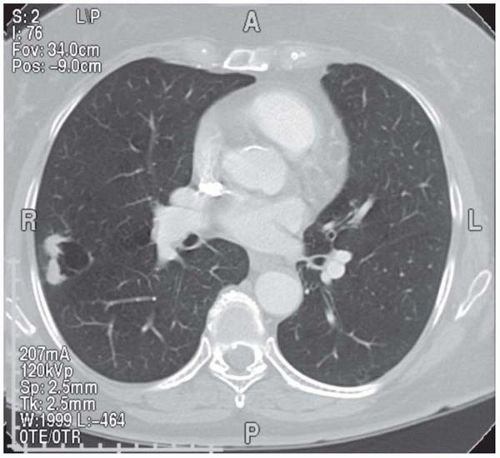 Figure 12.1 |
CT Scan Report
A 2.5-cm solitary pulmonary nodule is present in the posterolateral aspect of the right upper lobe. There is no mediastinal or hilar adenopathy seen. The CT scan includes cuts through the upper abdomen; both adrenal glands are visualized and appear normal, as does the liver.
▪ PET Scan
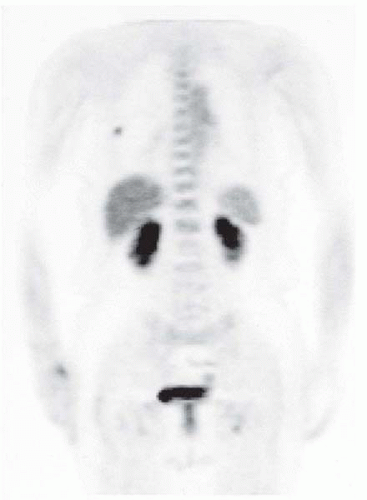 Figure 12.2 |
PET Scan Report
There is one area of moderate 5-fluorodeoxyglucose (FDG) accumulation within the right upper lobe nodule corresponding to the abnormality seen on the chest CT scan. The measured maximum standard uptake value (SUV) for the nodule is 2.5; this SUV value would be considered borderline with respect to malignancy.
Case Continued
The pulmonary function testing shows a forced expiratory volume at 1 second (FEV1) of 1.55 L or
69% of predicted. The diffusion capacity is 71% of predicted.
69% of predicted. The diffusion capacity is 71% of predicted.
The bronchoscopic examination is unremarkable, with no evidence of any mucosal abnormality or discrete endobronchial lesion. The cytology studies from the bronchial brushings and bronchoalveolar lavage show no evidence of malignancy.
Case Continued
The pulmonologist refers the patient for evaluation. On further review you find the patient to be quite healthy and very active. Her past surgical history is significant for 2 cesarean sections and a hysterectomy 24 years ago. She has no history of malignant disease but admits to a 40-pack-year smoking history, as mentioned previously. She has no palpable supraclavicular, cervical, or axillary adenopathy on examination. Her lungs are clear in all fields bilaterally and there is good air entry with no crackles or wheezes. She has no clubbing or cyanosis.
Differential Diagnosis
The differential diagnosis of a solitary pulmonary nodule is quite broad and can include both benign and malignant processes. Patient-specific factors, especially a smoking history, increase the probability that a solitary pulmonary nodule is malignant. Our patient, with her significant smoking history, has a high likelihood of harboring a primary carcinoma of the lung. In appropriate clinical settings, other possibilities include metastatic nodules from commonly encountered cancers, including breast, colon, thyroid, or renal cell carcinomas. Benign neoplasms of the lung, such as a hamartoma, can also be entertained but these lesions usually are evident on CT scan because of their characteristic “popcornlike” calcification pattern. Other possibilities include inflammatory or infectious nodules, the most common lesion being a granuloma. Several fungal diseases, including coccidioidomycosis and histoplasmosis, may present with a solitary pulmonary nodule, as may actinomycosis. The elusive rounded atelectasis, seen as a pleural-based lesion, may also appear to be a solitary pulmonary nodule.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


