Case 1
Presentation
A 56-year-old man presents to your office with a progressive painful ulcer of the tongue of 3 months’ duration. The lesion started as a painless ulcer, which gradually increased in size and became painful during the past week. He reports no history of similar ulcers or of trauma. He reports smoking cigarettes for the past 20 years; however, there is no history of alcohol abuse. Examination reveals a 4.5 × 3.5-cm indurated ulceroproliferative lesion of the left lateral border of the tongue. Tongue movement is normal. There is no extension of the induration to the base of the tongue or to the floor of the mouth. The rest of the oral mucosa appears healthy. There is no palpable cervical lymphadenopathy. A direct flexible laryngoscopy performed in the office reveals normal larynx and hypopharynx.
▪ Clinical Photograph
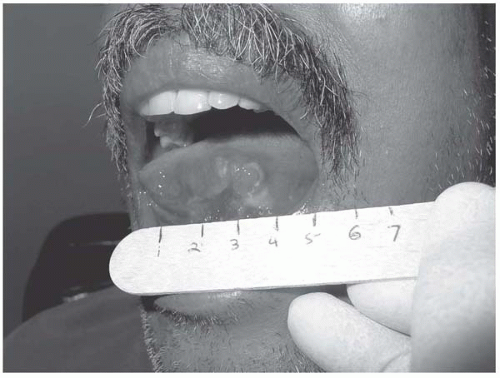 Figure 1.1 |
Physician Examination Report
Ulceroproliferative lesion of the left lateral border of the tongue.
Differential Diagnosis
Any oral ulcer that persists for more than 3 weeks should be considered malignant unless proved otherwise by biopsy. The painless nature of the lesion at onset and its increase in size further favor the diagnosis of a malignant lesion. The presence of induration on clinical examination is diagnostic of malignant lesions. However, because the patient complains of pain, it is necessary to exclude other reactive and inflammatory lesions. These include recurrent major aphthous ulcers and bullous lesions, such as pemphigus and pemphigoid, and the others listed later. The nonrecurrent nature of the lesion and presence of induration of the surrounding tissue make the diagnosis of reactive and inflammatory lesions less likely. Necrotizing sialometaplasia and keratoacanthoma, however, can mimic malignant ulcers. Other benign lesions likely to be considered are tuberculous ulcer and peripheral giant cell granuloma.
More than 90% of oral malignant lesions are squamous cell carcinomas. Other diagnoses to be considered are nonepidermoid malignancies (e.g., minor salivary gland tumors). These lesions usually have an intact overlying mucosa. In view of the relative rarity of other entities, the characteristic physical examination findings, and the risk factor of smoking, a provisional diagnosis of oral squamous cell carcinoma of the lateral tongue is considered for this patient.
Discussion
The oral tongue accounts for 20% to 50% of all squamous cell carcinomas of the oral cavity. Given their painless nature, they may grow considerably before a patient seeks medical help. On average, there is about 6 months’ delay in the diagnosis of oral squamous cell carcinoma by primary care physicians and dentists. Many of these patients are subjected to treatment by antibiotics prior to referral for definitive treatment. In this respect, considering biopsy of any oral lesions of more than 3 weeks’ duration is an important rule. Cervical nodal metastasis occurs
more frequently from cancer of the tongue than any other site within the oral cavity. More than 50% of patients present with a locally advanced lesion and lymph node metastasis. Even in patients without clinically obvious metastasis, there is over 30% risk of occult nodal metastasis. Biopsy of cervical lymph nodes is mandatory in establishing the diagnosis. Examination of other head and neck sites is mandatory to rule out synchronous tumors. Palpation of the tongue helps to delineate the submucosal extent of tumor and extension to the floor of the mouth and mandibular alveolus, which should be taken into consideration when planning surgical excision.
more frequently from cancer of the tongue than any other site within the oral cavity. More than 50% of patients present with a locally advanced lesion and lymph node metastasis. Even in patients without clinically obvious metastasis, there is over 30% risk of occult nodal metastasis. Biopsy of cervical lymph nodes is mandatory in establishing the diagnosis. Examination of other head and neck sites is mandatory to rule out synchronous tumors. Palpation of the tongue helps to delineate the submucosal extent of tumor and extension to the floor of the mouth and mandibular alveolus, which should be taken into consideration when planning surgical excision.
Differential Diagnosis Algorithm
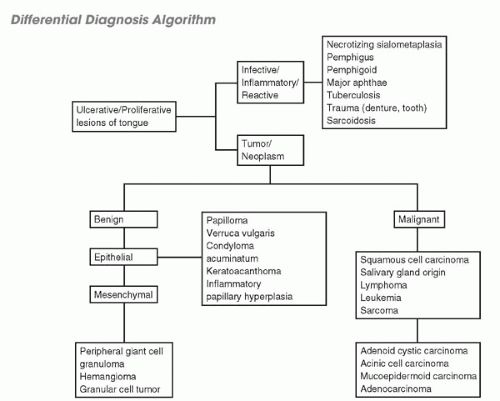 Figure 1.2 |
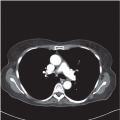
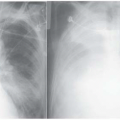
Recommendation
Computed tomography (CT) scan with contrast required to determine the extent of primary lesion and to evaluate the neck. Biopsy to confirm diagnosis.