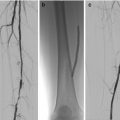
Figure 13.1
The patient with obvious cardiovascular risks
How to Tackle These Issues: Putting CV Risk Management at the Forefront of Diabetes Foot Care
The paradigm shift needed for CV risk management involves all providers of diabetes foot care services from foot screening, podiatry, wound care and multidisciplinary foot teams. The whole emphasis on saving more limbs needs to be re-balanced with the need to save more lives. Discussing CV risks along with limb risk, signposting patients towards medicine review (e.g., antiplatelet agents or intensified blood pressure control) or lifestyle change support (e.g., smoking cessation or weight management) and reviewing these issues on a regular basis is the responsibility of all clinicians working with diabetes foot disease.
Diabetes multidisciplinary teams and associated clinical services are made up of an eclectic mix of very highly skilled clinicians, often vying for individual clinical ideals. We must, however, unite on this theme to prioritise and deliver a single CV risk management approach and one set of simple consensus agreed CV targets. We must agree and clarify within our teams who is leading on and who shares responsibility for CV risk identification, management, review and discussion.
Amongst the plethora of limb-focussed diabetes foot literature, green shoots of CV-related emphasis are now emerging. For example, where multidisciplinary diabetes foot teams have systematically introduced aggressive CV risk factor management in people with foot ulcers, outcomes around 5-year mortality rates have been seen to dramatically improve, from 48 to 26.8 % [14]. Success in CV risk factor reduction in people with diabetes has also been demonstrated where nurse-led clinics have been set up to focus on the key modifiable risks [15].
Although there is a lack of direct clinical evidence to show the benefits of CV exercise in people with diabetic foot complications, the current norm of actively withdrawing or advising against this intervention surely must be one of our key priorities for change. Is it beyond our means to design, provide and actively promote prescribed, ‘low impact’, chair-based CV exercise for all our patients with foot disease, in particular those with foot ulcers, Charcot neuroarthropathy, or those who have already had an amputation. Could this not be done in partnership with existing cardiac rehabilitation services, to start to offer people with diabetes foot complications the same safe, supervised, effective exercise intervention, that their ‘cardiac cousins’ already have access to?
As a start point for clinicians wanting to tackle all these themes, simply discussing CV risks with patients can start to improve their perceptions, understanding and intent to initiate health changes [12]. An example of a CV risk discussion leaflet developed and used by a nurse and podiatry-led peripheral arterial disease service is shown in Fig. 13.2 [16]. This was based on gaining local clinician consensus and endorsement on CV targets sourced from a range of best national guidance (Fig. 13.3). Similar structured patient information, with simple numeric targets, linked to signposting towards available local support services could be developed by clinicians working with diabetes foot disease patients, to help achieve a balanced perspective on CV risks and the potential benefits of managing them better.
Figure 13.2
Example of a cardiovascular risk discussion leaflet used by a nurse and podiatry-led peripheral arterial disease service (Reprinted with permission from Pennine Acute Hospital NHS Trust)
Figure 13.3
Consensus endorsed CV targets, sourced from a range of best national guidance (Reprinted with permission from Pennine Acute Hospital NHS Trust)
Such a standardised multidisciplinary foot team approach to CV risk identification, discussion and targets can help to develop a common language and common goals, which can only help to reinforce key messages. Utilising the ‘seven components for ideal CV health’ as a common reference point and priority for continued professional development with all clinicians involved with diabetes-related foot disease, may help simplify the information, messages, language and targets we discuss with our patients.
Summary
Ultimately, taking the initiative at every opportunity to open the discussion on modifiable CV risk with our diabetes foot disease patients and to then touch base frequently on this theme in the context of their foot disease is a decision for individual clinicians to make. Only by starting the conversation will we ever really start to challenge existing lack of knowledge or inaccurate health-related beliefs and impact on the shocking mortality outcomes we see currently. Considering the effort that patients and clinical teams expend to achieve wound healing in the foot, it seems a great pity that many patients then suffer an avoidable cardiovascular death. It is no longer good enough to reassure ourselves that at least the patient died with both legs still on.
Related posts:
 Foot Deformity and Pressure Management in the Diabetic Foot
Foot Deformity and Pressure Management in the Diabetic Foot
 Screening and Treatment of Early Complications in the Diabetic Foot
The Role of the Multidisciplinary Team in the Management of Diabetic Foot Complications
Screening and Treatment of Early Complications in the Diabetic Foot
The Role of the Multidisciplinary Team in the Management of Diabetic Foot Complications
 Imaging in the Patient with Foot Complications
Imaging in the Patient with Foot Complications
 Neuro-osteoarthropathy: The Charcot Foot – Pathology, Diagnosis, and Treatment
Neuro-osteoarthropathy: The Charcot Foot – Pathology, Diagnosis, and Treatment
 Endovascular Revascularisation: When and How
Endovascular Revascularisation: When and How
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


