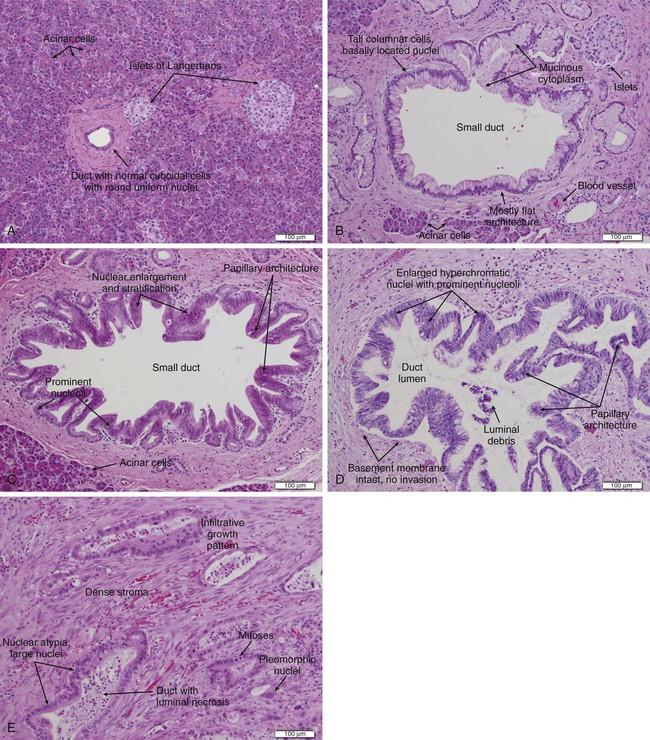
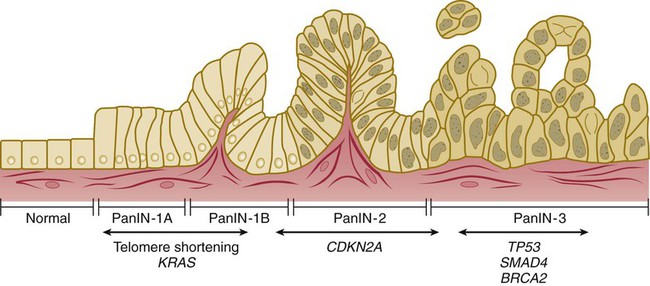
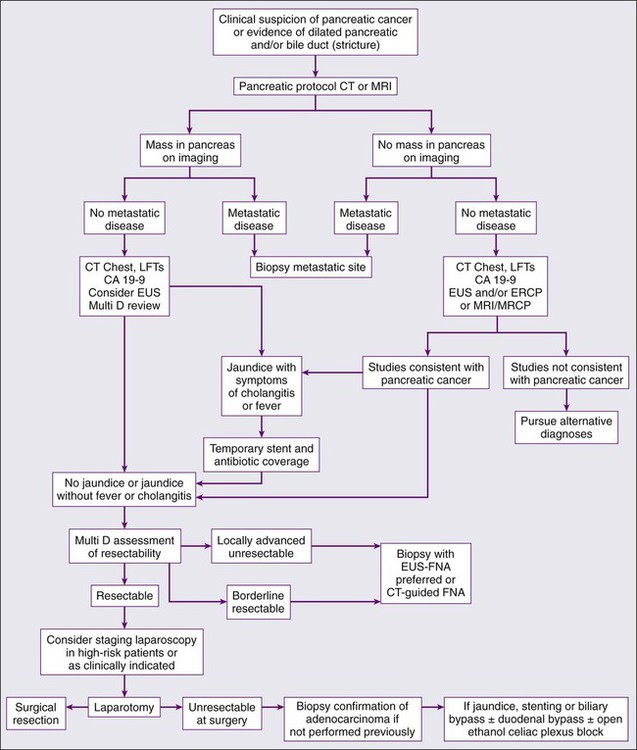
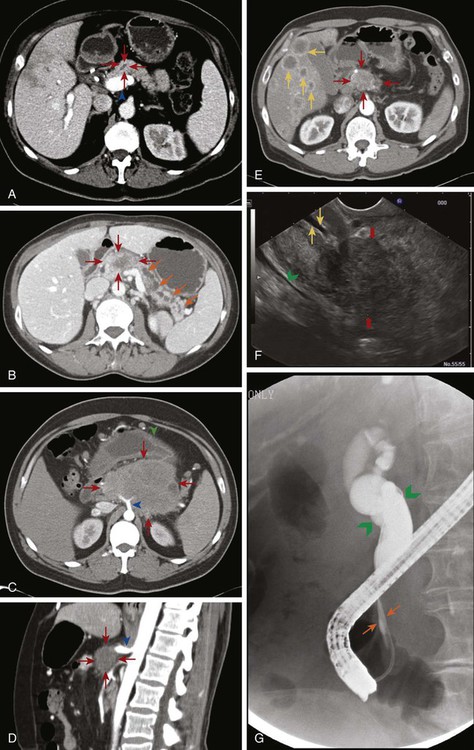
Lauren A. Mauro, Joseph M. Herman, Elizabeth M. Jaffee and Daniel A. Laheru • Pancreatic adenocarcinoma is the tenth leading cause of cancer in the United States, but the fourth leading cause of cancer-related deaths. • The overall 5-year survival for all patients is <5%: 15% to 20% of patients present with resectable/ borderline resectable disease with median survival of 20 to 24 months; 25% to 30% present with locally advanced/unresectable with median survival of 8 to 14 months; 50% to 60% present with metastatic disease with median survival of 4 to 6 months. • Familial atypical multiple-mole melanoma syndrome, hereditary pancreatitis, Peutz-Jeghers syndrome, and a strong family history of pancreatic cancer are the strongest risk factors and these patients should undergo screening. Risk factors also include smoking, heavy alcohol consumption, chronic pancreatitis, obesity and diabetes. • Screening of the general population is not indicated at this time. • Mutations in the KRAS oncogene and the CDKN2A tumor suppressor gene are found in more than 80% of pancreatic tumors and are thought to be early mutations. Inactivation of tumor suppressor genes TP53 and SMAD4 are thought to occur later in the tumorigenesis process. • Pancreatic intraepithelial neoplasms (PanINs) are microscopic precursor lesions. PanIN-3 lesions should be fully resected when found. Intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neoplasms (MCNs) are noninflammatory cysts that can lead to pancreatic cancer. All MCNs, main duct IPMNs, and symptomatic branch duct IPMNs should be resected. • Jaundice, abdominal pain, malabsorption, weight loss, back pain, and nausea/vomiting are common manifesting symptoms. • Pancreatic protocol computed tomography (or magnetic resonance imaging) should be used for diagnosing and staging. Endoscopic ultrasound may offer additional staging information. It is critical to determine resectability on imaging as that will determine the course of treatment. • All patients should be evaluated in a multidisciplinary setting when possible. • Surgery should be considered upfront in patients with resectable disease unless treated on a neoadjuvant clinical trial. • Patients should receive adjuvant 5-FU– or gemcitabine-based chemotherapy with 5-FU– or gemcitabine-based chemoradiation when appropriate as adjuvant therapy leads to longer survivals. • Neoadjuvant chemotherapy followed by chemoradiation can be given in patients with borderline resectable disease to increase the likelihood of R0 resections, treat micrometastatic disease earlier, and avoid surgery in patients who demonstrate early progression. • Locally advanced and metastatic disease patients can be treated with the same systemic chemotherapy regimens. Approved regimens include gemcitabine single-agent therapy, gemcitabine combination therapy, and 5-FU combination therapy. • Chemoradiation or stereotactic body radiotherapy can be considered for locally advanced patients with good performance status if there is no disease progression after initial systemic chemotherapy. • Palliative measures should be introduced early for advanced patients and focus on relieving pain, biliary obstruction, gastric outlet obstruction, and malnutrition. • Additional studies are needed to evaluate the ability of novel biomarkers to guide pancreatic cancer management. • Research focused on developing new therapies should take its cues from preclinical studies that are dissecting the stromal/tumor/inflammatory cascade of signals unique to pancreatic cancers. Pancreatic adenocarcinoma (PC) has one of the highest incidence-to-mortality ratios of any disease. Although it represents the tenth leading cause of cancer in the United States, it is the fourth leading cause of cancer-related deaths1 because the vast majority of patients will die from their disease. The overall 5-year survival for all patients with PC is less than 5%.4–4 This is in part because there is no appropriate screening test for the general population and manifesting symptoms are vague. Once patients are diagnosed, only 15% to 20% of patients present with resectable, and thus potentially curable, disease.2,5–8 However, even in the patients with early stage disease, median survival is 20 to 24 months with a 5-year survival of only 15% to 20%,2,7,9–20 as the majority will eventually recur despite surgery and adjuvant or neoadjuvant therapy. PC demonstrates complex biological features, presents with aggressive growth and is poorly responsive to chemotherapy. Patients with locally advanced (25% to 30% at presentation) and metastatic disease (50% to 60% at presentation) have median survivals of only 8 to 14 months and 4 to 6 months,2,5,7,21–28 respectively. However, some of the more recent trials with combination chemotherapy regimens provide some promise with improved survival in selected patients. As many patients suffer from biliary obstruction, diarrhea, pain, and malnutrition, palliative care can provide great benefit. While there has been improved understanding in the biology of PC translating in some modest improvements using contemporary chemotherapy and/or chemoradiotherapy, there are still significant gaps of understanding that must be identified in order to advance the treatment of this disease. This chapter reviews carcinoma of the exocrine pancreas, the most common form of cancers of the pancreas. In 2013, there will be an estimated 45,220 new cases and 38,460 deaths from PC in the United States alone,1 accounting for 12.1 new cases/year per 100,000 people. Worldwide, there are more than 278,600 new cases and more than 266,600 deaths per year, with an average of 4.1 new cases/year per 100,000 people. This rate does vary according to location, with more developed regions having a higher rate of 13.5 on average (Japan, Czech Republic, Hungary, and Finland have the highest rate of 18) as compared with an average rate of 2 for less developed regions (Africa and South-Central Asia have the lowest with <1 new case).29 These numbers are expected to increase as the world’s population grows and ages. The male-to-female ratio is virtually identical, with only a slight male predominance.29 This is a cancer of older adults, with the median age at diagnosis of 72 years in the United States, and with more than 66% of cases being diagnosed at an age older than 65 years. Only 2.6% of cases are diagnosed in persons younger than the age of 45 years and it is virtually never found in children. There are some racial disparities in the United States, as there is a slightly higher incidence in African Americans (17.5 new cases/year per 100,000 people) as compared with whites (13.5 new cases), Hispanics (11.4 new cases), and Asians (10.6 new cases; all incidences reported for men),30,31 and the age of diagnosis is younger in the African American and Hispanic groups.32 As PC is relatively uncommon yet incredibly aggressive, numerous risk factors have been identified that aid in preventative measures (Table 81-1). Cigarette smoking is one of the most clearly proven and most preventable risk factors. The risk increases with longer duration and higher number of cigarettes smoked, but can return to normal after 10 years of cessation.33,34 Cigarette smoke includes more than 50 carcinogens, the most important being nitrosamines, which promote tumor growth via various pathways, including activating the KRAS oncogene, and cause inflammation in the pancreas.35–35 It is believed to cause 15% to 25% of PC, with a relative risk of 1.5- to threefold in smokers as compared to nonsmokers.2,33–37 Chronic pancreatitis, often the result of chronic and heavy alcohol consumption or biliary duct blockages, leads to an increased risk of two- to 16-fold, although less than 5% of patients with chronic pancreatitis will develop PC. The chronic inflammation is thought to activate macrophages that produce cytokines that induce cell proliferation, angiogenesis, and inhibit apoptosis.34–36,38–42 Chronic pancreatitis may also be a manifesting symptom of PC from biliary obstruction caused by the tumor. Consequently, PC should be in the differential for a person who develops pancreatitis without any known risk factor.32,42,43 Patients with hereditary pancreatitis, caused by a mutation in PRSS1 in the autosomal dominant form leading to premature activation of trypsin while still in the pancreas as opposed to in the duodenum, or by a mutation in SPINK1 or CFTR in the autosomal-recessive form, have a 40- to 85-fold increased risk and a cumulative risk of 30% to 55% of developing PC in their lifetime.35,36,44,45 Alcohol is clearly a causative factor for cancers of the upper aerodigestive tract; however, it appears that only heavy alcohol use, defined as 3 or more alcoholic drinks per day, has a slightly increased relative risk of 1.2, whereas mild or moderate intake poses no increased risk.33,35–37 Obesity, defined as body mass index equal to or greater than 30 and accounting for 33% of adults in the United States, may lead to an increased risk of 1.2- to 1.7-fold and possibly higher in the severely obese.35,36,46 This link may result from increased circulating insulin and insulin growth factors, lower amounts of antiinflammatory cytokines, and a chronic low-grade inflammatory state throughout the bodies of obese people.46 The relationship between diabetes mellitus and PC is difficult to ascertain as type 2 diabetes can be both an early sign of PC and a risk factor. PC is thought to lead to diabetes through destruction of glands causing decreased production of insulin; however, the presence of diabetes does not appear to correlate with the size or stage of the tumor as this theory would suggest,47 so other mechanisms must be at play. Long-term diabetes is thought to increase the risk for PC because the increased secretion of insulin and insulin-like growth factors promote cell growth and the heightened state of inflammation leads to proinflammatory cytokines that contribute to angiogenesis and tumorigenesis.48 Studies have demonstrated that 55% to 85% of PC patients were diagnosed with glucose intolerance or diabetes either concurrently or within the 2 years preceding their cancer diagnosis.35,47,48 But, given the very high incidence of diabetes in the population, the relative risk of developing PC is still only 1.3- to 2.6-fold normal, when considered independently of obesity,35,37,47,48 and does not imply that all newly diagnosed diabetic patients warrant screening. However it should be considered in the atypical patient with newly diagnosed diabetes who has a steady or decreased weight, no change in activity and no family history of diabetes.36 Diets high in animal protein, history of gallstones, Helicobacter pylori infection, and some occupational exposures may lead to an increased risk.2,41,43,49,50 Allergies such as hay fever, increased vitamin D intake, blood type O, and diets high in fruits, vegetables, and citrus fruits may have a protective effect.2,35,36,44,51–54 Although the majority of PC are sporadic, 5% to 10% of patients have a family history.2,34,44 Familial PCc are defined as two or more first-degree relatives with the disease.35 Having one first-degree relative with PC gives a person a threefold increased risk, two first-degree relatives has a 4- to 6.4-fold increase risk, and three or more first-degree relatives poses a 14- to 32-fold increased risk.34,44,45 Although some patients with familial pancreatic cancer do not have identifiable genes, many syndromes have been described. Carriers of the BRCA2 gene (associated with breast, ovarian, and pancreatic cancers) have a 3.5- to 10-fold increased risk and account for 5% to 17% of families with familial PC. Mutations in PALB2 (binds to BRCA2) carry a sixfold increased risk,2,44 whereas BRCA1 carriers may have a twofold increased risk.2,35,36,44,55,56 Germline mutations in STK11 cause the autosomal dominant Peutz-Jeghers syndrome, characterized by hamartomatous polyps, pigmented macules, and a more than 90% chance of developing some form of cancer including a 132-fold increased risk for PC.2,35,36,44,50 Familial atypical mole-multiple melanoma patients typically have a mutation in CDKN2A and carry a 13- to 47-fold increased risk of PC.2,35,36,44,45 Germline mutations in DNA mismatch repair genes causing Lynch syndrome carry a two- to eightfold increased risk.35,36,44,57 Cystic fibrosis, characterized by a mutation in CFTR that produces viscous mucus that obstructs pancreatic ducts, carries an increased risk of 5.3-fold,35,44 whereas familial adenomatous polyposis (germline mutation in APC gene) has a four fold increased risk.44,45 Mutations in the tumor suppressor gene TP53 causing Li-Fraumeni syndrome results in a doubling of the risk.44 Understanding the molecular characteristics of PC is critical in order to aid in the development of targeted therapies. Several oncogenes and tumor suppressor genes are involved in the development of PC both by contributing to the growth of the tumor itself as well as to the support cells. Oncogenes, typically inactive in the normal cell, cause uncontrolled cell proliferation by inhibiting apoptosis and activating the cell cycle when mutations make them constitutively active. The KRAS oncogene, located on chromosome 12 and the most frequently mutated oncogene in PC (mutated in 80% to 90% or more of tumors), encodes a membrane-bound protein that has guanosine triphosphatase activity and is involved in signal transduction. When a mutation, typically a point mutation in codon 12, makes it constitutively active, its functions are independent of growth factors, which leads to chronic activation of its downstream pathways PI3K, MAPK, and RAF causing inhibition of apoptosis, activation of the cell cycle, migration, angiogenesis, cytoskeleton remodeling, and unchecked proliferation.5,35,45,54,58–62 When the AKT1 oncogene is activated through phosphorylation in the PTEN/PI3K/AKT pathway, it helps the cancer cells overcome cell-cycle arrest, blocks apoptosis, and promotes angiogenesis.35 Other oncogenes that are mutated in some pancreatic adenocarcinomas include BRAF (in KRAS wild-type tumors), MYC, MYB, and AKT2.45,54,59,60,62 Tumor suppressor genes, normally active, act in the opposite manner by activating apoptosis and inhibiting cell proliferation. However, tumor suppressor genes can be silenced when mutations make them inactive. CDKN2A, a cell-cycle control gene, is the most commonly inactivated tumor suppressor gene in PC, (lost in 80% to 95% of cases), leading to increased cell-cycle progression.5,35,45,54,60–62 TP53 is activated when there is DNA damage to either stop the cell cycle and repair the DNA or initiate apoptosis. Mutations in this tumor suppressor gene are found in 50% to 75% of tumors.5,35,45,54,58,61,62 Inactivation of SMAD4 (DPC4), involved in regulating cell cycle progression through the TGFB pathway, is seen in more than 50% of PC and is associated with worse prognosis and the development of metastases.5,35,45,54,58,62–64 Inactivation of RB1, in less than 10% of PC, and STK11, responsible for Peutz-Jeghers syndrome, is also seen.45,54 Other genes that have been demonstrated to be abnormal include the overexpression of IGF1, which leads to the abnormal activation of many downstream pathways, CDKN1A and CDKN1B mutations that cause loss of regulation at G1 checkpoint, EGFR TGFB mutations causing activation of MAPK pathway, and overexpression of ERBB2 (HER2/neu).58,62,63 There are several main signaling pathways involved in pancreatic tumorigenesis. The hedgehog signaling pathway, critical in embryogenesis, regulates the cell cycle and apoptosis, aids with the formation of the tumor stroma, and is often upregulated and abnormal in pancreatic cancers.54,61,63 The NOTCH pathway, also important in normal embryogenesis to prevent terminal differentiation of cells until appropriate, can be abnormally activated in pancreatic cancer, which allows cells to stay in an undifferentiated state contributing to tumor growth.54,63 When the WNT pathway, involved in maintaining the endocrine pathway, is activated, β-catenin is stabilized and migrates into the nucleus where it activates its target genes.35,54 The EGFR, TGFB, and JAK/STAT pathways have been found to be abnormal in PC cells leading to the promotion of cell growth, proliferation, differentiation and cell survival.35,54,63 The MET/HGF pathway is upregulated in most PC, and activates the downstream pathways including Ras, PI3K, JAK/STAT, and WNT, promotes angiogenesis and encourages cancer cell dissemination.35 NFKB1 proteins are a family of transcription factors that control numerous genes involved in inflammatory response, immune response, cell proliferation, apoptosis, differentiation and tumorigenesis. When its regulation is impaired, NFKB1 translocates into the nucleus and activates its target genes.54,63 Epigenetic modification, the process by which gene expression is altered by mechanisms other than changes in the actual DNA sequence, also has a role in PC tumorigenesis. DNA methylation and histone modification are two examples of this.2,45,65–67 Telomere shortening and overexpression of microRNAs lead to chromosomal instability and dysregulation of gene expression, respectively.2,45,58 In addition to the cancer cells themselves, the tumor microenvironment is comprised of stromal cells, inflammatory cells, and endothelial cells. The cancer cells secrete growth factors IGF1, FGF, TGFB, VEGF, and PDGFR that stimulate the pancreatic stellate cell (also called myofibroblasts) to secrete excess amounts of extracellular matrix. The matrix and its stromal cells in turn secrete cytokines and growth factors that promote cancer cell growth, invasion, and dissemination and protect the cancer cells from apoptosis. TGFB also leads to a decrease in activity of helper T cells, which suppresses the body’s immune system reaction against the abnormal cancer cells.5,54,58,63,68 Approximately 85% of PC develops from the ductal epithelial, termed pancreatic ductal adenocarcinoma (PDAC). PDACs are thought to arise from precursor lesions: pancreatic intraepithelial neoplasms (PanINs), intraductal papillary mucinous neoplasms (IPMNs), and mucinous cystic neoplasms (MCNs). PanINs, the most common precursor lesions, are defined as “microscopic papillary or flat noninvasive epithelial neoplasms [of <5 mm diameter, not visible by imaging] arising from the pancreatic ducts…characterized by mucin-containing cuboidal to columnar cells [with varying degrees of nuclear and architectural atypia].”45,62 PanINs, are classified from low-grade atypical lesions (PanIN-1A or -1B) to high-grade atypical lesions (PanIN-2 or -3) as molecular alterations accumulate and more dysplasia appears (Figs. 81-1 and 81-2).2,35,54,58,63,69,70,356 One reason for their identification as precursor lesions is the presence of similar mutations as compared with invasive carcinoma. Activating mutations of the KRAS oncogene are one of the earliest abnormalities in the development of PC, as they appear in 30% to 45% of PanIN-1 lesions and more than 90% of PanIN-3 lesions. BRAF mutations are also found in the early precursor lesions in the 5% of patients that are KRAS wild-type. Telomere shortening also occurs early and is present in 90% of PanIN-1 lesions and leads to chromosomal instability making further mutations more likely. Inactivating mutations of CDKN2A begin to occur in PanIN-2 lesions and inactivation of TP53, BRCA2, and SMAD4 are seen in PanIN-3 lesions.2,45,54,58–61,70 Low-grade PanIN lesions are common in older individuals; however, higher grade PanINs are typically seen in association with invasive cancer, especially in those with familial PC.2,71,72 Although all precursor lesions have a risk of progressing to invasive carcinoma, the risk is very low for PanIN-1 lesions and very high for PanIN-3 lesions, as patients with PanIN-3 lesions at the margins of a resection virtually all recur with invasive carcinoma. Consequently, it is recommended that all margins should be clear of PanIN-3, even if this requires re-resection.62,70 IPMNs and MCNs are two types of noninflammatory cysts in the pancreas that are diagnosed secondary to symptoms or from incidental findings on imaging. Cysts are found incidentally on 1.2% to 2.6% of the over 50 million computed tomography (CT) scans done annually in the United States. Given their malignant potential, recommendations have been developed for their management.73 IPMNs are grossly visible, mucin-producing, epithelial neoplasms, typically with papillary architecture, that arise from either the main pancreatic duct or branch ducts and are graded according to degree of dysplasia. They range from 5 mm to 150 mm, are more commonly located in the pancreatic head, and can manifest with abdominal or back pain, weight loss, or anorexia from ductal obstruction from the mucin or the tumor itself. The average age at onset is 65 years and they have a 2 : 1 male-to-female predominance. Endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) can visualize the degree of dilation of the main pancreatic duct to help determine the place of origin. They are less frequent precursors to PC than PanINs, but they do share some of the same molecular aberrations. KRAS mutations are seen in 50% of low-grade IPMNs, whereas inactivating mutations of CDKN2A and TP53 are seen in high-grade lesions. Loss of SMAD4 is only rarely seen in even high-grade lesions, while mutations of GNAS are commonly seen. IPMNs arising from the branch ducts are less aggressive than those arising from the main duct with rates of malignancy and invasive malignancy (either mucinous noncystic carcinoma/colloid carcinoma or PDAC) of 25% and 15% for branch duct origin and 70% and 43% for main duct origin. Patients with main duct IPMNs should undergo resection. Their 5-year survival rate is 77% to 96% for the noninvasive neoplasms and 40% to 70% in the invasive lesions. Symptomatic patients with branch duct IPMNs have a higher risk of malignancy and should undergo resection. Asymptomatic branch duct IPMNs can be monitored with imaging (every 3 to 12 months depending on size) as they have a 0% to 5% chance of malignancy, especially if there is no main duct dilation, no mural nodules and the neoplasm is smaller than 30 mm. They should be removed if they become symptomatic or increase in size. Patients should be followed even after resection as well, yearly for benign IPMNs and twice yearly for invasive IPMNs, to catch any recurrence.2,45,70,74,75 MCNs also produce mucin; however, they are characterized by ovarian-type stroma. They are found almost exclusively in women, typically in the fourth and fifth decades, and 95% are in the pancreatic body and tail. They tend to be slow growing, but the average size is 5 to 12.5 cm. They have an orangelike gross appearance and only rarely communicate with the pancreatic duct. All MCNs should be resected with a distal pancreatectomy and proper lymph node dissection as they may progress to mucinous cystadenocarcinomas which have a very poor prognosis. Patients with benign MCNs do not need to be followed after resection because they do not recur; however, patients with malignant MCNs (6% to 36%) should be followed by imaging every 6 months.2,45,70,74,75 Given the poor outcomes for patients diagnosed with PC, risk factor reduction and early detection are critical. Smoking cessation is the most important preventive measure and is strongly encouraged.2,33–37,76 Avoidance of heavy alcohol consumption can both reduce the risk of chronic pancreatitis, which is itself a risk factor, as well as reduce the carcinogens delivered to the pancreas from the alcohol.2,33–37 Decreasing the incidence of diabetes by maintain a healthy weight, a diet high in fruits and vegetables, and regular exercise will lower the risk.35–37,46–48,77,78 Unfortunately, the more severe risk factors are related to family history and congenital syndromes, which cannot be modified. Screening the general population is not feasible because of the relatively low incidence of PC and the lack of an inexpensive, accurate, and noninvasive test. A biomarker would be ideal for this situation, however, none have shown to be appropriate. CA19-9, a sialylated Lewis A blood group antigen, is the most studied biomarker that is expressed and shed in pancreatic and hepatobiliary diseases. It is often used after the diagnosis has been made in order to predict prognosis and chance of recurrence. However it is not a reliable screening tool for the general public as it can be elevated from other causes, such as cholestasis, cholangitis, pancreatitis, neuroendocrine tumors, and other gastrointestinal cancers, and 5% to 10% of people are nonsecretors as they do not express Lewis A antigen. As obstructive jaundice can falsely raise the CA19-9 value, it should be checked after biliary drainage if possible. Its sensitivity ranges from 80% to 100% and specificity from 68% to 98.5%.5,35,76,79–92 Although the positive predictive value is higher in symptomatic individuals, especially when combined with imaging, it cannot be used alone for screening. Individuals who are at high risk for developing PC, on the other hand, are recommended to undergo screening in order to catch premalignant lesions. The American Cancer of the Pancreas Screening (CAPS) Consortium did a prospective trial screening of high-risk individuals, defined as Peutz-Jeghers syndrome patients, familial breast-ovarian cancer patients with at least one affected first- or second-degree relative with PC, and relatives of patients with familial PC with at least one affected first-degree relative. They screened 225 high-risk individuals using CT, magnetic resonance imaging (MRI), and EUS, of which 82 had proven or suspected IPMNs and three had pancreatic endocrine tumors. Surgery was offered for suspected pancreatic neoplasms if there were solid masses, main duct or mixed duct IPMNs, branch duct IPMNs 2 cm or larger, or if there were concerning features. MRI and EUS was repeated in 6 to 12 months if lesions were found but no surgery was done, and repeated in 1 to 3 years if no mass was found. In the five patients who underwent pancreatectomy, all had high-grade dysplastic IPMN and/or PanIN but no invasive PC. The CAPS group considered this rate of identifying premalignant conditions adequate and recommended screening for this population starting at age 50 years, or 10 years before the earliest incidence in the family, or age 30 years for Peutz-Jeghers syndrome patients.93 The Fourth International Symposium of Inherited Diseases of the Pancreas also recommends screening high-risk individuals, defined as patients with greater than a 10-fold risk as per Table 81-1, as well as patients with three or more PC cases among first-, second-, and third-degree relatives, with at least one being a first-degree relative, and known BRCA1, BRCA2, and PALB2 mutation carriers who have at least one first- or second-degree relative with PC. Screening should start at age 45 years or 15 years before the earliest relative’s cancer onset, and should be done with EUS given its ability to detect pancreatic lesions smaller than 1 cm. Although MRI may be better, it has not been directly compared to EUS, and CT is less reliable for detecting small lesions.76,94 Several smaller studies have also demonstrated benefit of screening by finding precursor lesions in 8 of 72 high-risk individuals and 12 of 46 high-risk individuals,87,95 whereas others have shown only minimal yield.96 Therefore it is first recommended to test affected individuals in kindreds with familial PC for a causative mutation in order to properly test the unaffected individuals. Second, it is reasonable to screen high-risk individuals as defined per the studies above; however, it should be done in a clinical trial until randomized data proving its efficacy is available. Table 81-2 summarizes screening recommendations.2,35,44,58,76,93 Table 81-1 Risk Factors for Pancreatic Cancer FAMMM, Familial atypical multiple-mole melanoma; PC, pancreatic cancer. Table 81-2 The pancreas is composed of both exocrine and endocrine cells. The endocrine cells account for 1% to 2% of the pancreas and form the islets of Langerhans where they secrete insulin, glucagon, and somatostatin. The exocrine pancreas includes the acinar cells that produce and secrete digestive enzymes in their inactive forms, the cuboidal cells that line the smaller ducts, and the mucin-producing columnar cells that line the larger ducts which carry these enzymes to the duodenum. Fibroblasts, pancreatic stellate cells, endothelial cells, nerves, and inflammatory cells create the stroma surrounding the endocrine and exocrine pancreas.54,75 Of pancreatic epithelial neoplasms, 85% develop from the ductal cells and are identified by their glandular or ductal differentiation. These PDACs arise from the pancreatic head in 60% of cases, typically presenting earlier because they obstruct the distal common bile duct, the pancreatic body in 15% of cases, tail in 5%, and diffusely in 20%. Tubular adenocarcinoma is the most common histology; adenosquamous carcinoma, colloid carcinoma, hepatoid carcinoma, medullary carcinoma, signet ring cell carcinoma, undifferentiated carcinoma, and undifferentiated carcinoma with osteoclastlike giant cells are less common variants. Medullary and colloid variants have a better prognosis than the typical tubular adenocarcinoma, whereas adenosquamous and undifferentiated have an even worse prognosis. The remaining 15% of pancreatic epithelial neoplasms are composed of 1% to 2% serous cystadenomas, 1% to 2% MCNs, 3% to 5% IPMNs, 1% to 2% acinar cell carcinomas, less than 1% pancreatoblastomas, 3% to 4% pancreatic endocrine neoplasms, and 1% to 2% solid-pseudopapillary neoplasms.45,62,75,97,98 Invasive PC can spread through local invasion or through perineural, lymphatic, or vascular invasion, producing sites of distant metastasis. Given its location in the retroperitoneum, the most common sites of direct local invasion are to the stomach, duodenum, liver, common bile duct, gallbladder, spleen, superior mesenteric vein (SMV), superior mesenteric artery (SMA), and other surrounding arteries, veins, and lymph nodes. Perineural invasion is defined as the presence of cancer cells along nerves and/or within the neuronal sheath. Neurotrophins that are secreted by both the cancer cells and the nerve cells help support the survival and growth of these cells and promote neurogenesis, whereas chemokines like CX3CR1 appear to increase the cancer cells’ migration toward the nerve.99,100 The head of the pancreas is innervated by the superior mesenteric ganglion, the celiac plexus, and it branches which are the main routes for perineural invasion by the cancer cells. The main route of spread for cancers of the body and tail is through the celiac plexus and the splenic plexus. Intrapancreatic and/or extrapancreatic neural invasion is seen in virtually all advanced stage tumors, and even in more than 70% to 75% of stage I tumors, implying that this is an early event in the tumor’s progression. Given that some studies have reported worse prognosis for patients with perineural invasion, pathologists are now recommended to report the tumor’s perineural invasion status.99–105 In a retrospective analysis of 193 patients with resected PDACs, those without nodal metastases or perineural invasion had a 5-year survival of 75% as compared with 29% of those with perineural invasion. In patients with nodal metastases, 5-year survival was 17% when there was no perineural invasion and only 10% when there was invasion.103 Perineural invasion is one reason that many PC patients experience difficult to control abdominal and back pain.100 Vascular invasion is critical for both resectability and prognosis. The head and neck of the pancreas are supplied from superior pancreaticoduodenal arteries arising from the celiac trunk, and the inferior pancreaticoduodenal arteries arising from the SMA. These areas drain into the SMV, inferior vena cava, portal vein, and inferior mesenteric vein. The body and tail are supplied by the splenic artery arising from the celiac trunk and from pancreatic branches off the SMA and mostly drain into the splenic vein. Given their proximity to the pancreas, the SMV and SMA are the most commonly involved artery and vein by the tumor. The celiac artery, splenic artery, portal vein, hepatic artery, and, more rarely, the inferior vena cava and aorta can also be involved.6,106,107 On pathological review of more than 1100 resections, 53% had evidence of vascular invasion.108 Lymphatic invasion, and specifically nodal involvement, is the strongest predictor for survival. Lymphangiogenesis occurs during embryonic development and again during regeneration after a trauma and is thought to also occur during tumor growth. Tumor cells enter the lymphatic system by either migration through the interendothelial valves or by destroying the vessel walls. They will enter the smaller intralobular lymphatic vessels located within the pancreas and subsequently drain into the four main lymphatic branches of the pancreas: anterior, posterior, inferior, and superior pancreaticoduodenal lymphatic vessels. These then drain into regional lymph nodes that are typically located larger blood vessels: the celiac artery, common hepatic artery, SMA, and aorta for head/neck tumors and the splenic artery for body/tail tumors. At least 75% of all resections have positive lymph nodes.108–113 Tumor cells travel through the nerves, lymphatics, or vasculature to form distant metastases. The liver is the most common site of metastasis, possibly because tumor cells travel through the portal vein, followed by the peritoneal cavity. Lung metastases are the next most common, especially in long-term survivors.20,26,111,114–116 In a phase III trial for first-line metastatic PC, 88% of the patients had liver metastases, 24% had lung, 19% had peritoneal, and 14% had other sites.26 In a second-line therapy trial, 70% had liver disease, 30% had peritoneal, and 17% had lung involvement.116 Brain119–119 and skeletal metastases120 are quite uncommon and there have only been case reports of metastases to the appendix,121 kidneys,122 skin,123–126 prostate,127 stomach,128 heart,129 thyroid,130 and muscles.131 Although PC can cause numerous signs and symptoms, they often occur after the tumor is already at an advanced stage, making cure impossible and treatment challenging. When patients are diagnosed at early stages from incidental findings on scans, they can be asymptomatic.132 When the tumor has grown enough to cause biliary obstruction, symptoms include dark urine, light/clay-colored stool, pruritus, jaundice, scleral icterus, pancreatitis, and infectious complications such as cholangitis. As biliary obstruction typically occurs sooner for tumors of the pancreatic head, patients present with these tumors at an earlier stage than patients with body/tail tumors. Pancreatic enzyme insufficiency may cause malabsorption, increased flatulence, fatty stools, weight loss, and ascites. The pancreatic mass itself can cause compression or obstruction of the digestive tract, leading to nausea, anorexia, dyspepsia, pain, gastric or duodenal obstruction, and gastrointestinal bleeding. Pain may also be caused from perineural invasion or compression of the nerves surrounding the pancreas.2,5,88,98 It is usually dull, deep abdominal or middle back pain and is a poor prognostic sign, likely because of its association with larger tumors and micrometastatic disease.133 Approximately 85% of patients will have diabetes mellitus or glucose intolerance at diagnosis, with 55% to 85% of them being diagnosed within the preceding 2 years.35,47,48,134 Ten percent of patients may present with migratory thrombophlebitis with either deep or superficial venous thrombosis from the increase in procoagulants and platelet aggregation factors from the tumor.75 Many patients will report vague constitutional symptoms, such as generalized malaise, weakness, and depression, and most patients will report multiple symptoms at presentation.2,5,88,98 In several reviews describing the presenting symptoms of patients, 4.7% to 7% were asymptomatic, 34% to 51% had weight loss, 64% to 75% had jaundice, 39% to 55% had abdominal pain, 20% had back pain, and 13% had nausea/vomiting.98,108,135–137 When evaluating a patient for pancreatic cancer, it is recommended to involve a multidisciplinary team that includes medical oncology, surgical oncology, radiation oncology, pathology, and radiology.88,138 Figure 81-3 depicts a diagnostic algorithm. The goals of the imaging, labs, and biopsies are to help clarify the diagnosis, stage, resectability status, prognosis, and possible palliative options. As no patient should be denied a potentially curative surgery if the patient qualifies, the imaging of choice should emphasize specificity over sensitivity. Multiphase pancreatic protocol CT with IV contrast is typically the first study ordered (Fig. 81-4A-E). This should include a noncontrast phase as well as contrast-enhanced arterial (when tumor has poor enhancement as compared to pancreas parenchyma given its hypovascularity), pancreatic parenchymal, and portal venous phases, and include thin cuts of 3 mm or less to help detail the location of the tumor in relationship to the main vessels, find signs of mass effect or ductal obstruction, and detect small tumors and sites of metastasis.2,5,88,139–143 3D reconstruction can add additional information for surgeons planning the operation.88,142,144 CT has a 74% to 98% accuracy in detecting pancreatic cancer with sensitivities of 77% to 97% and specificities of 85% to 100%, with the lower numbers accounting for the smaller tumors that CT may miss because they have not caused any biliary or vasculature obstruction or impingement. Additionally, CTs have sensitivities of 55% to 97% and specificities of 91% to 100% for predicting vascular invasion, and sensitivities of 76% to 92% and specificities of 82% to 100% for predicting resectability. Typically, 10% to 30% of patients taken to surgery will have their surgery aborted or altered to a palliative only procedure because of more serious vascular involvement or metastatic disease that was not detected on CT scan.2,5,6,88,140–142,145–152 The technology has greatly improved and CTs have a higher accuracy now that the multiphase pancreatic protocols are being used. Chest CTs are also recommended to assess for pulmonary metastases prior to resection.2 Multiphase pancreatic protocol MRI can be used when CT is contraindicated and may be able to detect smaller lesions and better differentiate between cancer and pancreatitis. However, it hasn’t been shown to be superior to multiphase CT. MRI can also detail the biliary and pancreatic ductal systems via magnetic resonance cholangiography. Its sensitivities and specificities for diagnosis are 84% to 98% and 82% to 88%, and for predicting resectability are 82% to 88% and 78%, respectively.2,88,139,142,143,150,153–155 EUS is used in addition to either CT or MRI to obtain further information about nodal or vasculature involvement, to better identify suspected small lesions that were not seen on the prior imaging, and to help with staging (Fig. 81-4F). PDAC appears as a solid mass with irregular borders, is not homogeneous, and appears hypoechoic compared with the surrounding normal pancreatic parenchyma. Vascular invasion is determined when there is loss of the hyperechoic vessel wall and hypoechoic tumor interface, evidence of tumor within the vessel, irregularity of the vessel wall with tumor within 3 mm, inability to visualize a major vessel where collaterals are present, and vascular encasement. EUS may be superior to CT or MRI in differentiating cystic versus solid lesion, finding lesions smaller than 2 cm, noting pathological lymph nodes, and more accurately predicting the size of the tumor, but it is not very good at assessing SMA involvement. It does have the additional benefit of allowing a biopsy with fine-needle aspiration (FNA) or celiac plexus block to be performed at the same time. EUS has an accuracy of diagnosing PC of 86% to 96% with sensitivity of 85% to 100% and specificity of 98%.2,5,6,88,139,142,143,145,151,152,156–158 Although it is invasive, the complication rate is less than 2% and risk of major complications is 1 : 2500.159 Therefore EUS can be used as an adjunct to CT or MRI. ERCP combines endoscopy and fluoroscopy to map out the biliary system and may be beneficial if there is a duct stricture with no obvious mass as it does allow for ductal brushings. It also enables the placement of a biliary stent to decompress an obstructed system for patients who are receiving chemotherapy or for surgical patients who have a delay before surgery or have cholangitis (Fig. 81-4G).2,88,139,142,160 Positron emission tomography (PET)-CT may also be used in addition to pancreatic protocol CT or MRI to help clarify the presence of metastatic disease if this distinction would change management. With sensitivities of 85% to 100% and specificities of 67% to 99%, there can still be false negatives when tumors are smaller than 1 cm.2,5,6,88,142,161–163 Abdominal ultrasound, on the other hand, may be one of the first tests that is ordered to evaluate jaundice or abdominal pain and can demonstrate a hypoechoic mass or biliary dilatation, but it cannot firmly differentiate between PC, neuroendocrine tumor, and chronic pancreatitis. The addition of color Doppler does aid in detecting vascular invasion, but its accuracy of diagnosis is around 75%. Consequently, this will always need to be followed by further imaging.6,164–166 The use of staging laparoscopy has changed over time. It has been used in patients in whom unresectable disease is considered likely in order to prevent a larger laparotomy procedure that would need to be aborted. These higher-risk patients are those with CA19-9 higher than 100, head tumors larger than 3 cm, questionable findings on CT, or a body/tail lesion. Past studies did demonstrate that laparoscopy can prevent unnecessary laparotomies in 20% of patients, however these numbers are dropping to 5% to 8% as imaging studies have gotten better, making laparoscopy less likely to be helpful.6,88,139,167–169 Although a biopsy is not required when a patient with a high suspicion for PC goes directly to surgery, it is required prior to any neoadjuvant treatment or treatment of locally advanced or metastatic disease. FNA via EUS or CT-guidance are the two most common approaches to obtain a tissue sample. EUS-FNA is preferred because of the higher diagnostic yield, lower chance of seeding the peritoneum causing carcinomatosis, and the benefit of additional staging information from EUS. EUS-FNA has a 92% accuracy of correctly diagnosing a pancreatic mass and a 84% accuracy when performed in patients with negative CT-guided biopsies. It also carries a low complication rate of 0.5% to 2%.2,88,139,145,148,160,170–173 CT-guided FNA may also be performed to biopsy a metastatic site. ERCP brushings may also be done and should be considered when there is a biliary stricture but no mass, but cytology from brushings has a low yield of positive results.88,160 Although tumor-associated markers like CA19-9 can also assist in the diagnosis, as discussed previously, the sensitivity and specificity lead to a fair number of false positives and false negatives. The absolute value is often higher in more advanced stages, especially when there are liver metastases,86 and the value can provide useful prognostic information. Classically, PC has been staged according to the TNM (tumor–node–metastasis) staging system per the American Joint Committee on Cancer, as shown in Table 81-3.174 The distinction of T1 and T2 tumors at 2 cm is secondary to the association of tumor size with survival in resected patients. Numerous reviews have demonstrated improved survival in patients with smaller tumors with 5-year survival improvements by 10% to 20% and increase in median survival by 5 to 20 months and hazard ratios around 1.6. Unfortunately, only a minority of patients (6% to 25%) present with tumors smaller than 2 cm.8,98,101,108,175–181 The classification of patients with nodal disease separately as stage IIB is because of the clear associated of nodal disease with worse survival, as described further below.175 Table 81-3 TNM Staging for Pancreatic Carcinoma per Seventh Edition of AJCC174 More recently, most centers and current clinical trials are classifying patients based on their resectability status (Table 81-4) because surgery is critical to achieve a cure in this disease. This characterizes stage I and II patients as resectable and divides stage III patients into those who are borderline resectable and may benefit from neoadjuvant therapy prior to surgery from those who are unresectable and are not surgical candidates. Tumors that encase the SMA or celiac artery would require technically difficult resections and reconstructions that carry a high perioperative mortality risk and are likely to leave some tumor behind and are therefore categorized as unresectable. In addition, there is a greater chance of perineural infiltration with SMA or celiac artery involvement because those arteries have a perineural sheath unlike the SMV or portal vein.88,139,175 Tumors involving the SMV and portal vein are considered borderline resectable, on the other hand, because SMV and portal vein resection does not affect surgical outcome or overall survival when done at experienced centers and therefore is not an absolute contraindication to surgery.19,175,182 Unfortunately, only 15% to 20% of patients present with resectable or borderline resectable disease. Table 81-4 Classification of Resectability of Pancreatic Cancer per the National Comprehensive Cancer Network and Surgical Oncology Expert Consensus Statement2,5,7,21–28,88,139,175 Surgery is required to achieve a cure in patients with PC with resectable disease and improves overall survival. Patients with resectable tumors that undergo resection have a significantly longer survival of 20 to 24 months as compared with 10 to 12 months for patients with resectable tumors who do not have a resection.175 It is recommended that they be performed at a high-volume institution given the lower rate of operative mortality and morbidity.2,183 Resections are classified as R0 resections when the margins are clear of tumor, R1 resections where there is microscopic evidence of tumor at the margin, and R2 resections if there is grossly visible tumor at the margin. All attempts should be made to achieve an R0 resection as positive margins are a poor prognostic sign. There are three main surgeries for PC. The most common is a pancreaticoduodenectomy (Whipple procedure), indicated for pancreatic head tumors (Fig. 81-5). Prior to any resection, patients are first explored for resectability by evaluating for metastatic disease to the liver, peritoneum, or other viscera, examining the celiac and small bowel lymph nodes, and palpating the SMA, SMV, and portal hepatis.184 The surgeon will then resect the pancreatic head, distal bile duct, most of the duodenum, and proximal jejunum en bloc, described as a pylorus-preserving technique. At times, the remainder of the duodenum and gastric antrum must be resected to achieve a clear margin or when the duodenum is ischemic.108
Carcinoma of the Pancreas
Introduction
Epidemiology
Risk Factors
Etiological and Biological Characteristics
Molecular Biology
Precursor Lesions
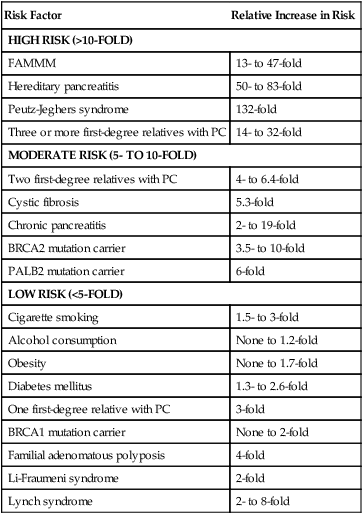
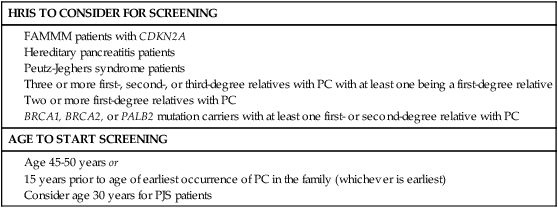
Prevention and Early Detection
Risk Factor
Relative Increase in Risk
HIGH RISK (>10-FOLD)
FAMMM
13- to 47-fold
Hereditary pancreatitis
50- to 83-fold
Peutz-Jeghers syndrome
132-fold
Three or more first-degree relatives with PC
14- to 32-fold
MODERATE RISK (5- TO 10-FOLD)
Two first-degree relatives with PC
4- to 6.4-fold
Cystic fibrosis
5.3-fold
Chronic pancreatitis
2- to 19-fold
BRCA2 mutation carrier
3.5- to 10-fold
PALB2 mutation carrier
6-fold
LOW RISK (<5-FOLD)
Cigarette smoking
1.5- to 3-fold
Alcohol consumption
None to 1.2-fold
Obesity
None to 1.7-fold
Diabetes mellitus
1.3- to 2.6-fold
One first-degree relative with PC
3-fold
BRCA1 mutation carrier
None to 2-fold
Familial adenomatous polyposis
4-fold
Li-Fraumeni syndrome
2-fold
Lynch syndrome
2- to 8-fold
Pathology and Pathways of Spread
Pathology
Pathways of Spread
Clinical Manifestations, Patient Evaluation, and Staging
Signs and Symptoms
Diagnosis
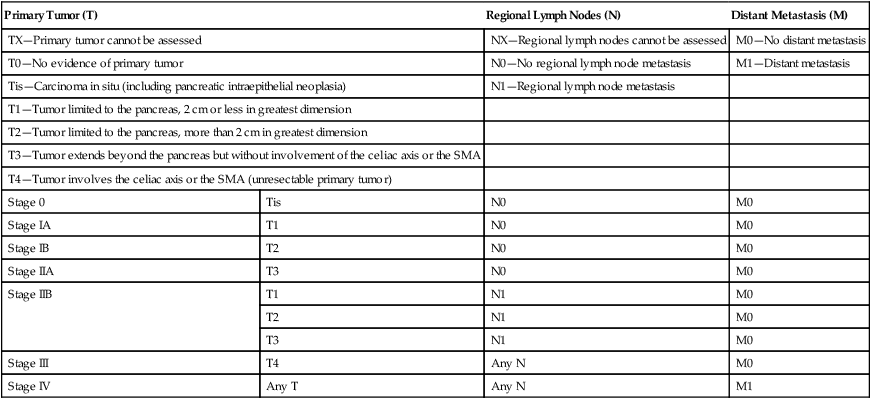
Staging
Primary Tumor (T)
Regional Lymph Nodes (N)
Distant Metastasis (M)
TX—Primary tumor cannot be assessed
NX—Regional lymph nodes cannot be assessed
M0—No distant metastasis
T0—No evidence of primary tumor
N0—No regional lymph node metastasis
M1—Distant metastasis
Tis—Carcinoma in situ (including pancreatic intraepithelial neoplasia)
N1—Regional lymph node metastasis
T1—Tumor limited to the pancreas, 2 cm or less in greatest dimension
T2—Tumor limited to the pancreas, more than 2 cm in greatest dimension
T3—Tumor extends beyond the pancreas but without involvement of the celiac axis or the SMA
T4—Tumor involves the celiac axis or the SMA (unresectable primary tumor)
Stage 0
Tis
N0
M0
Stage IA
T1
N0
M0
Stage IB
T2
N0
M0
Stage IIA
T3
N0
M0
Stage IIB
T1
N1
M0
T2
N1
M0
T3
N1
M0
Stage III
T4
Any N
M0
Stage IV
Any T
Any N
M1
Resectability Status
Criteria
Median Survival
Resectable
No distant metastases; no radiographic evidence of SMV and portal vein abutment, distortion, tumor thrombus, or venous encasement; clear fat planes around the celiac axis, hepatic artery and SMA (Fig. 81-4A)
20–24 months
Borderline resectable
No distant metastases; venous involvement of the SMV/portal vein demonstrating tumor abutment with or without impingement and narrowing of the lumen, encasement of the SMV/portal vein but without encasement of the nearby arteries, or short segment venous occlusion resulting from either tumor thrombus or encasement but with suitable vessel proximal and distal to the area of vessel involvement, allowing for safe resection and reconstruction; gastroduodenal artery encasement up to the hepatic artery with either short segment encasement or direct abutment of the hepatic artery without extension to the celiac axis; tumor abutment of the SMA not to exceed >180 degrees of the circumference of the vessel wall (Fig. 81-4B)
20 months
Unresectable/locally advanced
HEAD: No distant metastases; >180 degrees SMA encasement or any celiac abutment; unreconstructable SMA/portal occlusion; aortic invasion or encasement
BODY: No distant metastases; SMA or celiac encasement >180 degrees; unreconstructable SMV/portal occlusion; aortic invasion
TAIL: No distant metastases; SMA or celiac encasement >180 degrees
ALL: Metastases to lymph node beyond the field of resection (Fig. 81-4C and D)
8–14 months
Metastatic
Any presence of distant metastases (Fig. 81-4E)
4–6 months
Primary Therapy
Surgery
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oncohema Key
Fastest Oncology & Hematology Insight Engine






