Cancer-related fatigue (CRF) is one of the most prevalent symptoms reported by cancer patients and survivors—and one that presents many challenges. Most epidemiologic studies of fatigue indicate that it occurs more frequently and more severely than other symptoms in patients with cancer during the course of their disease and its treatment, regardless of the type of cancer or type of therapy; one 1997 study described the fatigue seen in patients with cancer as “both pervasive and profound” (1). In another study, a significantly greater percentage of cancer patients than healthy individuals reported severe fatigue (rated 7 or higher on a 0 to 10 scale) (2). CRF may persist even among cancer survivors who have no evidence of active disease (3,4).
Such findings evidence the importance of establishing a standardized method for assessing and managing fatigue in routine clinical oncology care (5,6). Efforts to develop educational and research initiatives that would help patients and health care providers better understand fatigue and help clinicians better treat fatigue began about a decade ago; since then, knowledge of CRF has progressed, allowing new hypotheses to be generated for further study. Nonetheless, knowledge about the pathophysiologic mechanisms of CRF is limited, and an effective intervention in oncology patient care has yet to be established.
In this chapter, we define CRF, summarize the available research on clinical factors and underlying mechanisms of CRF, discuss methodological issues in measuring CRF and interpreting fatigue assessment results, and review innovations in CRF intervention.
DEFINING CRF
Although fatigue is reported to be the most common symptom of cancer, definitions of CRF have varied from study to study. However, many definitions of CRF share similar features, describing CRF as physical, subjective, temporal, emotional, cognitive, unusual, and affecting the patient’s ability to function. Table 7.1 shows a review of these 7 characteristics of CRF, distilled from 24 definitions considered by the working group “Assessing the Symptoms of Cancer using Patient-Reported Outcomes” (ASCPRO) (7). ASCPRO defined CRF as the “perception of unusual tiredness that varies in pattern and severity and has a negative impact on ability to function in people who have or have had cancer” (7). Similarly, the well-known and accepted National Comprehensive Cancer Network (NCCN) guidelines on fatigue define CRF as “a persistent subjective sense of tiredness related to cancer or cancer treatment that interferes with usual functioning” (8).
Fatigue could be described clinically with a range of terms, such as weariness, exhaustion, lassitude, weakness, malaise, discomfort, impatience, and the inability to perform aspects of normal functioning. Although patients with CRF use a variety of phrases to describe their fatigue, more often than not they characterize themselves as “suffering” from fatigue. However, the distinction between patient perception of CRF and that of “typical” fatigue remains somewhat vague. CRF may be ever-present or transient (a “fatigue attack,” in which its onset is more rapid than that of typical fatigue). CRF also lasts longer, drains more energy, and is more severe and unrelenting than typical fatigue. Because CRF overlaps with multifactorial physical and psychological disorders (e.g., depression), it has been recognized as falling into “muddy water” conceptually. The European Association for Palliative Care has recognized both a physical and a cognitive dimension to fatigue and recommends that screening for fatigue include both a question about weakness to cover the physical dimension and a question about tiredness to cover the cognitive dimension (9).
Data from qualitative studies could help create a simplified approach to understanding CRF. For example, a qualitative study compared the key domains of adaptation for “tired,” “fatigued,” and “exhausted” in patients with cancer, suggesting that behavioral changes in sleep quality, stamina, cognition, and emotional reactivity may serve as early markers of impending fatigue and that decreased control over body processes and reduced social interaction may be signs that an individual has entered a state of fatigue (10). A recent review and synthesis of qualitative research on CRF between 1996 and 2009 identified concepts and language used by patients to describe CRF (11). In this study, patient quotes suggested that the word “tiredness” does not adequately capture the multidimensional nature of the CRF experience.
TABLE 7.1 Characteristics of fatigue
Characteristics
Terms Indicative of the Characteristics
% Definitions Including Characteristics
Subjective
Self-report, self-perception
58
Physical sensation
Severity of sensations, including exhaustion, decreased energy, weakness, malaise, tiredness, lassitude
92
Unusual
Unrelieved by rest, unusual, abnormal, not proportional to activity, unusual need for rest, unpredictable
42
Impact on functioning
Decreased function, decreased capacity for work, decreased quality of life, difficulty completing tasks, poor sleep quality, withdrawal from activities, debilitation
CRF negatively affects a patient’s daily functioning and can diminish the quality of life. It can be so overwhelming that patients elect to discontinue treatment, or oncologists may give patients a “chemo holiday” to recover from severe symptom burden. A quantitative study found that CRFrelated interference with functioning, as measured by the Brief Fatigue Inventory, helped differentiate fatigue severity levels (2). In this study, an increase in a patient’s worstfatigue rating was associated with an increase in the fatigue’s interference with patient function. When the worst fatigue reached 6 or greater on the Brief Fatigue Inventory’s 0 to 10 scale, its interference with all aspects of daily life was moderate to severe (4 or higher on the 0 to 10 scale) (12).
CLINICAL FACTORS IN CRF
The NCCN guidelines attribute the causes of CRF to both the cancer and the cancer therapy (8). CRF can occur during any phase of the disease, and it often results from a combination of cancer progression and the body’s acute or late response to cancer therapy, plus the impact from other medical and psychological conditions and chronic illness.
Disease-related CRF is often observed in patients newly diagnosed with cancer. Unusual tiredness is frequently the first indicator that something is amiss (13). In a study of elderly patients newly diagnosed with various cancers, higher levels of fatigue were found in patients with late-stage disease than in patients with early-stage disease and with lung cancer (14). In patients with advanced cancer, tumor progression affects multiple organ systems and causes neurologic and physiologic changes in skeletal muscle that are potentially relevant to CRF.
Cancer therapies, especially chemotherapy, can induce CRF and exacerbate existing CRF (5,15,16,17,18). A history of chemotherapy was independently associated with severe CRF in patients with various types of advanced cancer (19). Chemotherapy-related toxicities, such as hematologic, gastrointestinal tract, and neural toxicities, may also increase the CRF severity. For some chemotherapy regimens, CRF is an expected adverse event, and patients receiving such regimens as standard care during acute treatment often accept CRF as the price they must pay to achieve a cure. For patients undergoing maintenance therapy (such as patients with chronic myeloid leukemia receiving long-term imatinib therapy), CRF is often a critical factor in deciding whether or not to withdraw from treatment.
Other cancer therapies, such as surgery, radiotherapy, stem cell transplantation, and immunotherapy, can also induce or exacerbate CRF. Patients with cancer often experience postoperative fatigue immediately after a curative surgical procedure, although increased analgesia has been shown to attenuate immediate postsurgical fatigue (20). Gradual increases in fatigue severity have been observed during radiotherapy or concurrent chemoradiation (5,15,16,17,18). Radiotherapy can induce anemia, diarrhea, anorexia, weight loss, and chronic pain, any of which may be associated with an increase in CRF. When high-dose chemotherapy is paired with stem cell transplantation, patients experience a dip in white blood cell count after the transplant, which has been found to be associated with a peak in fatigue levels (21,22). Biological response modifiers, such as proinflammatory cytokines and hormones, are also known to produce CRF. Administration of interferon (IFN)-α can cause flu-like symptoms and has been shown to produce fatigue in 70% of patients (23). In patients with breast cancer, hormone treatment has been associated with lethargy and lack of energy equivalent in severity to the postradiotherapy fatigue experienced by patients with prostate cancer during hormone treatment (24). In addition, fatigue is one of the most common side effects of many tyrosine kinase inhibitors (25). Even though fatigue is a well-known issue for cancer patients and survivors, CRF was not noted among a list of adverse drug reactions that occurred after initial labels for targeted anticancer agents were approved on the basis of randomized phase III clinical trials (26), and there are no existing data on the impact of CRF-related drug discontinuation on disease control.
Even for cancer survivors who have completed therapy and have no evidence of active disease, CRF can be a persistent and functionally bothersome symptom. A populationbased survey of 1-year cancer survivors revealed that fatigue was 1 of 3 most negative symptoms (along with depression and pain) among 67 symptoms affecting health-related quality of life (27). Fatigue is also perceived to be a significant problem in child and young adult cancer survivors. Meeske et al. (28) found that 30% of 161 long-term survivors of acute lymphoblastic leukemia whose cancer was diagnosed before the age of 18 years reported having fatigue and that fatigue was highly associated with depression. In a multicenter study of 1,897 adult long-term survivors of childhood cancer (those who had a cancer diagnosis before age 21 and survived at least 5 years after the diagnosis), the overall prevalence of CRF was 19% among all survivors and 15% among the acute lymphoblastic leukemia survivors, after adjustment for medical and socioeconomic factors, including depression (29). Survivors were significantly more fatigued than their siblings. Survivors with fatigue were also more likely to experience depression than were survivors who did not have fatigue. These findings indicate that long-term follow-up care should include psychological assessments and interventions for childhood cancer survivors at highest risk (30).
Research over the past decade has revealed that acute physiologic conditions (which may or may not be related to cancer or cancer therapy), chronic medical conditions and their treatments (e.g., pain, disturbed sleep, decreased activity levels, infections, anemia, nutritional deficiencies, dehydration, electrolyte disturbances, cardiac deconditioning, pulmonary disorders, neuromuscular disorders, thyroid dysfunction, liver failure, renal insufficiency, and diabetes), psychosocial stress and emotional distress (e.g., anxiety, depression, and environmental reinforcers), and concurrent exposure to sedating medications (e.g., opioids) can also contribute to CRF in patients with cancer, although the exact nature of these influences cannot be determined. In addition, most patients with cancer are of advanced age, increasing the likelihood that they suffer from comorbidities that are also risk factors for CRF.
POTENTIAL UNDERLYING MECHANISMS OF CRF
Several descriptive studies have carefully documented the development of fatigue and how it interacts with potential biological mechanism targets in specific cohorts. However, numerous challenges exist in the translational area of the biomedical sciences for narrowing down host factors related to CRF. Thus, little progress has been made in identifying a biomarker that could serve as an objective measure of fatigue. Few neuroimaging studies have examined CRF expression in the human brain, and animal models representing CRF have not been established. Translational work is needed to find a mechanism-driven intervention for fatigue.
CRF does not develop in all patients at risk for it. Studies of genomic encoding for CRF are now beginning to explore the increased activity of proinflammatory transcription factors as contributors to fatigue in cancer survivors. In a study using genome-wide expression microarrays, Bower et al. (31) reported increased expression of inflammation-related genes, particularly those responsive to the proinflammatory nuclear factor-κB transcription control pathway, together with decreased expression of glucocorticoid-dependent antiinflammatory genes between breast cancer survivors who had persistent fatigue and nonfatigued controls. However, Reinertsen et al. (32) found no association between persistent fatigue and the expression of either single nucleotide polymorphisms in inflammation-related genes (interleukin [IL]-1β, IL-6, IL-6 receptor, and C-reactive protein genes) or mRNA IL-1β and IL-6 receptor in a large sample of breast cancer survivors, even after excluding depressed individuals.
Patients with cancer—especially those undergoing aggressive therapy, those with advanced disease, and those who have accompanying medical comorbidities or psychological disorders—rarely experience just one severe symptom. CRF often accompanies a cluster of other moderate to severe symptoms, such as pain, distress, poor appetite, drowsiness, and disturbed sleep. In a large case-controlled study of survivors with breast cancer, depression and pain were the strongest predictors of fatigue (3). This suggests that a complex interplay exists between the etiological agent (e.g., cancer treatment, infections, and use of centrally acting drugs) and the patient’s susceptibility to fatigue.
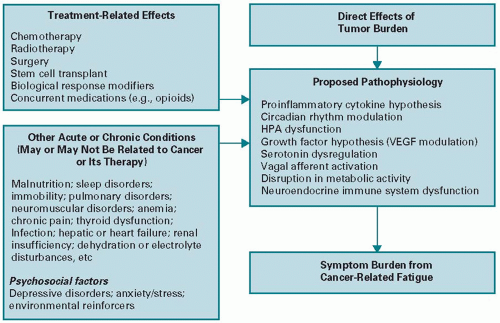
However, the lack of clear pathophysiologic explanations hampers our ability to determine whether a constellation of mechanisms causes CRF or whether a centrally mediated disorder characterized by CRF exists. Although the underlying etiology of fatigue is not yet fully understood, several working hypotheses to explain the mechanisms of this complex phenomenon have been suggested. Figure 7.1 presents the proposed etiologies of CRF.
The proinflammatory cytokine hypothesis, one of the primary proposed explanations of CRF, suggests that dysregulated inflammation and its toxic downstream effects constitute a significant biological basis for CRF and other cancer-related symptoms (13,21,33,34,35,36,37). As a typical nonspecific symptom in patients with cancer, fatigue is similar to certain sickness behaviors observed in animal models in studies of the behavioral effects of cytokine administration (38). Basic research on activation of immune-to-brain communication pathways in response to continued activation of the peripheral immune system indicates that proinflammatory cytokine (mainly IL-1β and tumor necrosis factor [TNF]-α) signaling to the brain leads to an exacerbation of sickness in vulnerable individuals, who develop a constellation of behavioral changes that include fatigue, disturbed sleep, and symptoms of depression (37). Increased expression of positive acute-phase proteins such as C-reactive protein and decreased expression of negative acute-phase proteins such as albumin are also highly correlated with persistent CRF (39). Certain inflammatory biomarkers (IL-6 and TNF-α) were identified in vivo and in vitro (40); these biomarkers are associated with activation of innate immune cells and T-cells (41).
The role of activation of the proinflammatory cytokine network in fatigue and other symptoms has been under investigation since the 1990s, although the relevance of these findings is limited by few translational studies confirming the results. In a quantitative review and meta-analysis of 18 studies, Schubert et al. (42) found that CRF was associated with increased circulating levels of IL-6, IL-1 receptor antagonist, and neopterin. Reductions in fatigue were observed in patients given antagonists of TNF-α as an intervention for improving the tolerability of chemotherapy (43). More recently, clinical studies have indicated that TNF-α signaling plays a role in postchemotherapy fatigue in patients with early-stage breast cancer (44). A temporal association was also found between serum or plasma inflammatory markers induced by aggressive cancer therapy and the development of fatigue and a cluster of other sickness symptoms (pain, disturbed sleep, drowsiness, and poor appetite) that affect physical functioning in patients with cancer (21,45,46). Inflammatory processes associated with tumor growth can cause abnormalities in energy metabolism and inhibit muscle function: Inagaki et al. (47) found that elevated levels of plasma IL-6 were associated with increased levels of fatigue in terminally ill patients with cancer.
The development of a spectrum of symptoms of depression in response to cytokines is well established in both animal models and humans, especially in the context of cytokine immunotherapy (48,49,50,51). Current research indicates that proinflammatory cytokines can cause depression in several ways, including glucocorticoid receptor resistance in immunocytes and their cellular targets through the activation of signalling pathways such as p38 mitogen-activated protein kinase and jun-N terminal kinase. This culminates in activation of the tryptophan-degrading enzyme indoleamine 2,3-dioxygenase, which generates neurotoxic metabolites (52). In cancer patients treated with IFN-α, hypermetabolism in the left putamen and nucleus accumbens, likely related to reduced dopaminergic transmission, was associated with fatigue and lack of energy (53).
Only gold members can continue reading. Log In or Register to continue