48 Cancer of the Uterine Cervix
Epidemiology
It was estimated that 11,270 new cases of invasive carcinoma of the uterine cervix would be diagnosed in the United States in 2009, representing 1.6% of all cancers in women.1 An estimated 4070 deaths from cervical cancer were expected in 2008, accounting for 1.5% of all cancer deaths in women. The average age for patients with invasive disease is in the mid- to late 40s, with approximately 25% of cases and 50% of deaths occurring in patients older than 65. At the time of presentation, 45% of cases are localized, 34% have regional spread, and 10% have disseminated disease.
During the last five decades, the incidence of invasive cervical carcinoma has dropped dramatically, from 32.6 (late 1940s) to 8.3 (mid-1980s) per 100,000 women in the United States.2 Much of this improvement is attributable to the development of effective screening techniques for the identification of preinvasive lesions. Incidence varies worldwide, with the highest rates found in Latin America and the lowest prevalence found among Jewish women in Israel. Over the past decade, there has been a noticeable increase in the incidence of preinvasive lesions reported in many nations, and an actual increase in mortality rates in young women in Canada, Great Britain, New Zealand, and Australia.2
Lower socioeconomic status is associated with an increased risk of frankly invasive disease, partially because of ineffective or absent screening programs in many parts of the world.3 Although in developed nations there appears to be an increased incidence among black and Latino people as compared with white or Asian people Surveillance Epidemiology End Results (SEER) data from 1987 showed that black people had twice the incidence of invasive cervical cancer as white people, socioeconomic factors cloud the issue.2 When evaluated in a multifactorial analysis, race drops significantly as a major factor.
As of January 1, 1993, the Centers for Disease Control and Prevention modified their reporting guidelines to state that the presence of cervical carcinoma in the setting of infection with the human immunodeficiency virus (HIV) establishes the diagnosis of acquired immunodeficiency syndrome (AIDS), regardless of CD4 count or absence of prior opportunistic infections. The incidence of infection with human papillomavirus (HPV) is higher in HIV-positive women than their HIV-negative counterparts. Likewise, because T-cell immunity is essential in maintaining control of HPV infection, an increase in the incidence of cervical intraepithelial neoplasia (CIN) and invasive cervical carcinoma is seen in this population.4
Two strains of HPV (16 and 18) are considered to have a high malignant potential, whereas strains 31, 33, 35, 39, 40, 45, 51-56, and 58 have a moderate malignant potential. HPV DNA sequences are identified in 80% to 100% of cervical carcinomas evaluated by polymerase chain reaction.4 In June 2006, the Food and Drug Administration (FDA) approved the first preventive HPV vaccine (quadrivalent HPV recombinant vaccine [Gardasil]). In 2007, the FDA approved a second HPV vaccine (HPV bivalent vaccine [Cervarix]). In a 5455-patient, randomized, placebo-controlled, double-blind trial, the vaccine showed 100% efficacy against cervical lesions and external anogenital and vaginal lesion in the patients who completed the vaccination regimen.5 The adverse events associated with the vaccine were mild to moderate. Serious adverse events occurred in less than 0.1% of patients. The vaccine is currently not licensed to use in female patients younger than 9 years or older than 26 years, or for male patients. Proposals for compulsory vaccination are currently being evaluated in various states.
Attention has returned to the role of herpes simplex virus type 2 (HSV2) as a potential cofactor with HPV in the initiation of malignant degeneration.2 Women with HSV2 alone have a 1.2 relative risk (RR) compared with women negative for both HPV and HSV2. Those positive for HPV16/18 DNA alone had an RR of 4.3, but those positive for HPV 16/18 and HSV2 had an RR of 8.8.
Early age at initiation of sexual activity and multiple sexual partners are associated with increased risk.2 Girls who begin engaging in intercourse before the age of 16 have a twofold increase in risk over those who begin after age 20. Exceptionally low rates are found in Catholic nuns and Mormon and Amish women. Cigarette smoking has been implicated,2 with most studies revealing a twofold increase in incidence in smokers compared with nonsmokers. Multiple dietary elements are currently being investigated for their potentially protective effects, including vitamins A, C, and E, as well as beta-carotene.
Diethylstilbestrol (DES), a nonsteroidal estrogen developed in the 1940s and used in the prevention of recurrent or threatened miscarriages, was administered to between 0.5 and 2 million women in the United States before it was banned for this purpose by the FDA in 1971. Intrauterine exposure to DES was found to be associated with the development of clear cell adenocarcinoma of the cervix and vagina.6,7 In reports from the Registry for Research on Hormonal Transplacental Carcinogenesis, 60% of 519 cases of clear cell adenocarcinoma of the vagina or cervix were found to be related to exposure to DES or related compounds, with an estimated risk after exposure of 1 in 1000 up to the age of 34.8 Ninety-one percent of patients were diagnosed between the ages of 15 and 27, with more than 90% presenting with early (stage I or II) disease.
Anatomy
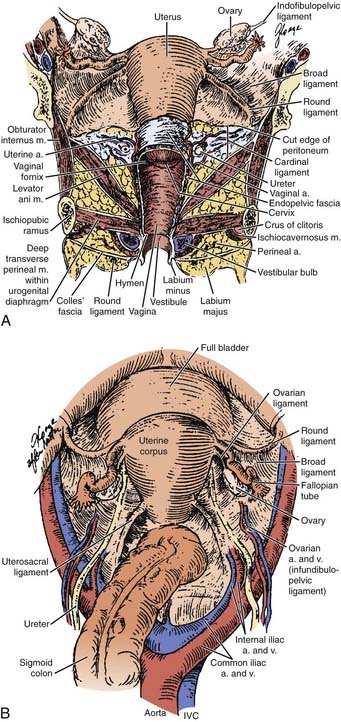
A clear understanding of the anatomic relationships of the uterine cervix and surrounding structures is essential for maximizing the therapeutic ratio in the management of cervical carcinoma. The cervix is sandwiched between the trigone of the bladder, the ureters, the anterior wall of the rectum, and the sigmoid colon, so that these critical organs are by necessity exposed to the interventions used to control neoplasms of the cervix (Fig. 48-1). The uterus itself is a hollow muscular organ divided functionally into two parts, the fundus and cervix, separated by a constriction known as the isthmus. The upper portion, the body or corpus uteri, is covered by the reflection of the peritoneum, which anteriorly becomes the peritoneal reflection over the bladder and posteriorly extends down over the cervix and posterior fornix of the vagina before covering the anterior portion of the rectum and sigmoid colon. The broad ligament is a double layer of peritoneum through which the blood supply, lymphatics, and nerves of the uterus course. These ligaments connect the lateral aspects of the uterus with the pelvic side walls. They contain three ligaments: (1) the round ligament anteriorly, which courses out through the abdominal inguinal ring; (2) the ovarian ligament posteriorly connecting the uterine pole of the ovary and the lateral uterus; and (3) the suspensory ligament of the ovary between the two layers of the broad ligament connecting the lateral pole of the ovary and the pelvic side wall. Atop the broad ligament lie the fallopian tubes. The ovaries are located posteriorly.
The lymphatics of the cervix course in three separate routes (Fig. 48-2). Laterally, they pass along the uterine artery to the external iliac lymph nodes. Posterolaterally, they pass behind the ureters to the internal iliac nodes. Posteriorly, they enter the common iliac and lateral sacral nodal groups. The fundus of the uterus drains mainly to the internal iliac nodes via lymphatics in the broad ligament, although some drainage occurs to the para-aortic chain via the ovarian vessels, to the external iliac chain, and to the inguinal nodes via the round ligament. The upper vagina drains laterally to both the internal and external iliac nodal groups, whereas the middle third tends to drain to the internal iliac group alone. The lower third of the vagina has lymphatic channels that merge with those of the vulva and lead to the superficial inguinal region. Depending on the local growth characteristics of cervical tumors, therefore, involvement of the internal and external iliac, para-aortic, sacral, and inguinal nodes is possible and must be taken into consideration when a treatment strategy is planned.
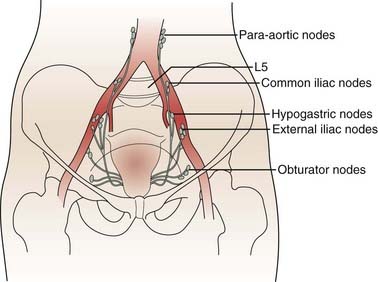
FIGURE 48-2 • Lymphatic drainage of cervix.
(From Crook J, Esche B: The uterine cervix. In Cox J: Moss’ radiation oncology, ed 7, St Louis, 1994, Mosby, p 618.)
Pathologic Conditions
In 1988, the National Cancer Institute convened a workshop to develop modern guidelines for cytopathologic reporting of cervical and vaginal specimens to replace the outdated Papanicolaou (Pap) classification, resulting in the Bethesda classification system for cytopathology reports (Table 48-1).9 For those lesions considered to be possible precursors of invasive carcinoma, the previously used CIN (levels I, II, III) and dysplasia (mild, moderate, severe, carcinoma in situ [CIS]) grading systems were replaced with a two-tier designation. Low-grade squamous intraepithelial lesions (LGSILs) include those lesions previously referred to as cellular changes associated with HPV infection or mild dysplasia (CIN I). High-grade squamous intraepithelial lesions (HGSILs) include moderate or severe dysplasia (CIN II or III) or CIS.
Table 48-1 Bethesda System for Reporting Cervical/Vaginal Cytologic Diagnoses
CIN, Cervical intraepithelial neoplasm; HGSIL, high-grade squamous intraepithelial lesion; HPV, human papillomavirus; LGSIL, low-grade squamous intraepithelial lesions; SIL, squamous intraepithelial lesions; WNL, within normal limits.
From NCI Workshop: The 1988 Bethesda system for reporting cervical/vaginal cytologic diagnoses, JAMA 262:931, 1989.
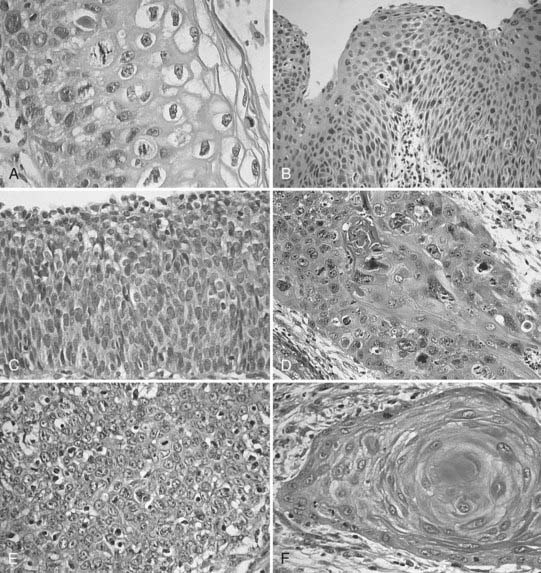
Invasive cervical cancers comprise approximately 85% squamous cell varieties, 15% adenocarcinomas, and a rare collection of other entities. Squamous cell carcinoma (SCC) has been classified according to a new system by the International Society of Gynecological Pathologists to include keratinizing, nonkeratinizing, verrucous, papillary transitional, and lymphoepithelial types (Table 48-2).10 Adenocarcinomas include the following subtypes: mucinous (endocervical, intestinal, and signet ring types), endometrioid, clear cell, minimal deviation (adenoma malignum), papillary villoglandular, serous, and mesonephric. The remaining tumor types include adenosquamous, glassy cell, adenoid cystic, adenoid basal, carcinoid, small cell, and undifferentiated carcinomas (Fig. 48-3).
Table 48-2 Histopathologic Type
From American Joint Committee on Cancer: Cervix uteri. In Fleming ID, Cooper JS, Henson DE, et al, (eds): AJCC Cancer Staging Manual, ed 6, Philadelphia, 2002, Lippincott-Raven.
Squamous Cell Carcinoma
Several different classification systems have been suggested during the past 60 years, including the early Broders/Warren classification (based on differentiation, mitotic activity, keratinization, and pearl formation) and that of Reagan and Ng (based on size, keratinization, and nuclear pleomorphism).11 In an analysis of patients entered into the Gynecologic Oncology Group (GOG) prospective treatment protocol for stage IB cervix carcinoma, none of the histologic grading systems for SCCs were found to correlate with incidence of lymph node metastasis or progression-free interval.12
Variants of SCC of the cervix exist, although it is unclear that any of these variations affect response to therapy. Verrucous carcinoma is a very well-differentiated carcinoma lacking cellular atypia and possessing orderly elements of maturation. It can achieve massive exophytic proportions and be extensively invasive, in contrast to the bland microscopic appearance. Verrucous carcinomas are differentiated from condylomata by the presence of invasion in addition to a lack of fibrovascular cores in the papillae, as well as by the exophytic expansion of surrounding normal tissue.11,13 Spread to lymph nodes is quite rare. Concern is expressed by many authors that the use of radiation in these lesions may contribute to malignant degeneration, but this point is contestable.14
Papillary squamous cell differs from the verrucous form in that its cells show a high degree of nuclear atypia. Although grossly the tumor may have a warty, exophytic appearance, on microscopic examination there are found papillae with atypical immature basaloid cells reminiscent of transitional cell carcinoma of the bladder. The determination of invasion requires full-thickness biopsy, because a large exophytic component may be associated with a minimal amount of invasion.11
Adenocarcinoma
Adenocarcinomas account for 10% to 20% of cervical neoplasms in the literature.15 This appears to represent an increase from older data that showed the incidence to be in the range of 5% to 10%, possibly because of a decline in the incidence in invasive SCC secondary to effective screening programs, although the possibility remains that the incidence of adenocarcinoma is actually on the rise. The most common type, endocervical adenocarcinoma, generally is composed of mucin-producing glands of varying differentiation, within a fibrous stroma that sets it apart from normal endometrial stroma. It may be difficult to differentiate from adenocarcinoma of uterine corpus origin, increasing the necessity of a proper fractional dilatation and curettage (D&C) to establish the actual origin of the disease. It appears in an admixture with other variants in a frequent number of cases.
Minimal deviation adenocarcinoma is a variant that is an extremely well-differentiated lesion composed of endocervical glands with basal nuclei and low nuclear/cytoplasmic ratios.16,17 The nuclei appear minimally atypical, belying the aggressive clinical nature. On extensive sampling, markedly dysplastic cells can be identified. These malignant glands can be helpful in differentiating these lesions from other benign conditions such as adenomatous hyperplasia or deep nabothian cysts. They are almost uniformly deeply invasive and are associated with a very poor prognosis. A high frequency of associated mucinous tumors of the ovary has also been reported.
Villoglandular papillary adenocarcinoma is generally found in younger women (average age 33) and consists of a surface papillary component with fibrous stroma.17 Unless there is clear evidence of vascular involvement or deep invasion, conservative management may be warranted owing to the excellent prognosis.
Endometrioid adenocarcinoma of the cervix is difficult to distinguish histologically from uterine adenocarcinoma. The clinical activity is similar to the endocervical variety.15,18
Clear cell adenocarcinomas of the cervix, most commonly seen in young women exposed to DES in utero, are identical to the lesions that show up in the vagina, endometrium, and ovary. They can be seen in women of any age in the absence of DES exposure history. Three patterns have been described (tubulocystic, solid, and papillary), with the appearance of cells bearing a “hobnail” configuration that clearly sets them apart from other variants of adenocarcinoma.6,8,19
Serous papillary adenocarcinoma is a rare subtype, which histologically looks similar to its namesake in the uterus and ovary.20 A search must be carried out to ensure that it is not a metastatic deposit from another site in the pelvis. Too few cases have been reported to state whether or not this entity in the cervix is prone to intraperitoneal dissemination like the uterine variety. Mesonephric, signet ring cell, and intestinal-type adenocarcinomas are additional extremely rare subtypes, for which care must be taken to rule out metastases from other locations.15
Adenosquamous and Glassy Cell Carcinoma
Adenosquamous carcinomas are tumors that contain mucin or glands in an admixture with clearly recognizable squamous elements.15,21 Any pattern of squamous cell may appear in this setting, usually in conjunction with poorly differentiated adenocarcinoma. Once again, care should be taken to establish that this is truly adenosquamous carcinoma and not two separate primary tumors of the cervix and corpus (“collision” tumors). A particularly aggressive form of poorly differentiated adenosquamous carcinoma is the glassy cell carcinoma, so called because of a ground-glass appearance to the finely granulated cytoplasm in conjunction with clearly defined cell walls and large nuclei with prominent nucleoli.21,22 These tumors, representing approximately 1% to 2% of all cervical neoplasms, have a high mitotic rate and a particularly aggressive course.
Small Cell (Neuroendocrine) Carcinoma
Small cell carcinoma is a neuroendocrine tumor similar to small cell tumors of the lung, believed to arise from amine precursor uptake and decarboxylation cells.23 It accounts for less than 2% of all cervical neoplasms. These lesions may have been lumped in with other small cell variants of squamous cell in the classification of Reagan mentioned earlier, giving rise to the differences seen in clinical outcome using that schema. Histologically, however, the picture seen is a sea of small monomorphous cells with a high nuclear/cytoplasmic ratio, with an occasional minimal element of glandular or squamous differentiation. Neuroendocrine granules may be identified on electron microscopy or immunohistochemical analysis. Up to one half may stain for markers such as serotonin, adrenocorticotrophic hormone, somatostatin, or gastrin, although clinical syndromes associated with the production of these markers is very unusual. A hallmark of this disease is its systemic nature early in the course of the disease. Any meaningful intervention must take into account the high propensity for early dissemination and include chemotherapeutic approaches similar to those used for oat cell carcinoma of the lung.
Other rare cervical tumors include carcinoid, adenoid basal, adenoid cystic, sarcomas (mixed müllerian, endocervical stromal), embryonal rhabdomyosarcoma, and melanoma. The interested reader is referred to the excellent review article by Clement.24 Although uncommon, the cervix may also be a site of metastatic disease.
Clinical Presentation
Extensive data support the theory that malignant lesions arise from the precursor lesions described as HGSIL. On reviews of earlier biopsies of patients found to have invasive disease, severe dysplasia and CIS are often found. Similarly, patients followed with serial biopsies after discovery of HGSIL show subsequent development of frank invasion. The two lesions are often found concurrently in specimens, and both arise most frequently from the squamocolumnar junction or the transformation zone.25 Most significantly, however, incident rates and death rates resulting from invasive cancer of the cervix have dropped dramatically during the past years in those regions where effective detection and treatment of HGSIL occurred.
Once the disease has broken through the basement membrane, the possibility of metastatic spread exists. Carcinoma of the cervix is divided into microinvasive (minimally invasive) or invasive. The former, making up approximately 10% of all carcinomas of the cervix, is defined as any tumor with no evidence of vascular or lymphatic invasion and less than or equal to 3 mm deepest invasion below the superficial stromal-epithelial interface. The depth of invasion necessary to satisfy the criteria for this diagnosis has been the subject of considerable controversy, varying from 1 to 5 mm, with most authors preferring the 3 mm mark, because lesions with this degree of invasion have less than 1% risk of lymph node metastases. In cases with invasion from 3.1 to 5 mm, 12 of 146 patients (8%) had pelvic lymph node metastases at lymphadenectomy.26 Although technically not a part of the definition of microinvasive carcinoma, the extent of lateral spread of the tumor has considerable prognostic significance, with lesions greater than 7 mm being associated with a greater lymph node metastatic rate.27
Dissemination of disease occurs either mainly through lymphatic channels or hematogenously, although intraperitoneal spread may occur in advanced disease. The lymphatic spread of disease tends to be orderly and predictable with internal and external iliac nodes first involved, followed by common iliac and para-aortic spread. Involvement of the lower third of the vagina is associated with spread to the inguinofemoral lymph nodes. The incidence of nodal involvement is correlated significantly with the stage and volume of local disease, as well as depth of invasion (Table 48-3).28 Stage I disease has an 11% to 18% risk of pelvic nodal involvement; stage II, 32% to 45%; and stage III, 46% to 66%.28 Para-aortic nodal involvement can also be associated with early stage disease and has been found to be a powerful prognosticator. The incidence of para-aortic nodal involvement is 0% to 18% for stage IB/IIA disease, 13% to 33% for stage IIB, up to 46% for stage III disease, and as high as 57% for stage IVA disease.29–31
Table 48-3 Incidence of Positive Pelvic Nodes
| Stage | I | 11%-18% |
| II | 32%-45% | |
| III | 46%-66% | |
| Depth of invasion | ≤3 mm | <1% |
| 3-5 mm | 1%-8% | |
| ≤5 mm | <1%-3.5% | |
| 6-10 mm | 15.1% | |
| 11-15 mm | 22.2% | |
| 16-20 mm | 38.8% | |
| >20 mm | 22.6% | |
| Maximum tumor dimension (IB/II) | 0.1-1.0 cm | 12.7% |
| 15.8 cm | 1.1%-2.0% | |
| 2.1-3.0 cm | 16.3% | |
| ≤3 cm | 21% | |
| >3 cm | 23%-42% | |
| Grade | 1 | 9.7% |
| 2 | 13.9% | |
| 3 | 21.8% | |
| Lymphovascular space invasion | Absent | 8.2% |
| Present | 25.4% |
Prognostic Factors
Tumor volume is directly related to the incidence of spread to pelvic and para-aortic lymph nodes, as well as inversely related to local control and actuarial survival. In a retrospective review by Piver and Chung30 of 289 patients who underwent a radical hysterectomy for stages IB, IIA, or recurrent cervical carcinoma at Roswell Park, patients with tumors 3 cm or less had a 21% incidence of pathologically involved nodes, compared with 35% to 42% for those patients with tumors greater than 3 cm. In a prospective GOG surgical pathologic study of patients with stage I SCC of the cervix treated with a radical hysterectomy and pelvic lymph node dissection, tumors up to 1.0 cm in maximum diameter had a 12% incidence of involved pelvic lymph nodes, compared with 23% for those tumors greater than 3 cm.32 A separate analysis of patients entered into three consecutive radiation trials for stage I-IVA cervical cancer by the GOG found tumor size to be a significant predictor for progression-free interval.33
In a retrospective review of 625 patients with stage IB-IIB cervical cancer treated with a radical hysterectomy between 1965 and 1977, Inoue28 found a significant correlation between the depth of invasion and the incidence of pelvic nodal involvement and parametrial involvement. Of 97 tumors less than 5 mm deep, there was only one with pathologic evidence of involvement of pelvic nodes. Other investigators have reported that tumors measuring less than 3 mm in maximum depth have a less than 1% risk of spread to pelvic lymph nodes,26 whereas tumors in the range of 3 to 5 mm deep have up to an 8% incidence of nodal involvement.34 Depth of invasion was a potent prognosticator for spread to pelvic lymph nodes in the GOG surgical pathologic study of patients with stage I cancer (P < 0.0001).32
Despite its imperfections, the International Federation of Gynecology and Obstetrics (FIGO) staging system has been effective in dividing patients into groups with different prognoses. The FIGO report of 8538 patients treated with either radiation or surgery between 1982 and 1986 showed the following 5-year actuarial survival rates: stage I, 81.6%; stage II, 61.5%; stage III, 36.7%; stage IV, 12.1%.35 According to the Patterns of Care Study, 5-year survival rates for stages I, II, and III cancers of the cervix treated with radiation were 74%, 56%, and 33%, respectively.36 The French Cooperative Group report in 1988 stated survival rates of 89% for patients with stage IB disease, 85% for IIA, 76% for IIB, 62% for IIIA, 50% for IIIB, and 20% for stage IV.37
Metastatic disease in the pelvic nodes is a powerful prognostic factor, as evidenced by multivariate analyses in both retrospective and prospective reports. The presence of disease in pelvic lymph nodes in stage I disease decreases the survival into the 50% to 60% range.28,30,38,39 In the Annual Report of the FIGO results in cervical cancer, patients with stage IB disease with negative nodes had an 89.5% 5-year survival versus 59% for those with histologically positive nodal involvement.35 In a retrospective review of 875 patients with stage IB-IIB resected cases found survival rates of 89%, 81%, 63%, and 41% for patients with no nodes, 1 node, 2 to 3 nodes, and 4 to 18 nodes positive, respectively.38 In the GOG analysis of patients treated with definitive radiation, the presence of para-aortic adenopathy was found to be the most potent prognostic factor evaluated.40
Anemia has been associated with decreased local control in patients with locally advanced cervical carcinoma in many series.41,42 The issue is quite complex because of the varying level of hemoglobin used to define anemia and the association of anemia with more advanced disease at presentation.43 In a multivariate analysis of prognostic factors in a retrospective review of 2800 patients with cervical carcinoma of all stages treated for cure performed at Princess Margaret Hospital, Bush found that anemia achieved a high level of significance, particularly at levels below 12 g/dl.44 It is not clear, however, that performing transfusions on patients to bring them up to a hemoglobin level of 12 g/dl alters outcome. In prospective study from the Princess Margaret Hospital, 132 patients with stage IIB or III disease were initially randomly assigned to either receive transfusions to keep their hemoglobin above 12.5 or not receive transfusions until the hemoglobin fell below 10 g/dl.44 Patients in either arm with hemoglobin greater than 12.5 did not receive transfusions. A subgroup analysis done retrospectively showed a significant decrease in local failure and disease-specific death rates for patients who received transfusions to keep their hemoglobin above 12 compared with anemic patients who did not receive transfusions. This information, although suggestive of a benefit for transfusion, is not conclusive. Several authors have failed to find a correlation between anemia and response to radiation. The suggested benefit of correction of the anemia must be weighed against the attendant risks of routine transfusions.41 Prior to the initiation of radiation, it is reasonable to correct severe anemia (hemoglobin less than 10 g/dl), or to transfuse the patient with borderline anemia who continues to actively bleed while attempts are made to control the bleeding with packing, the use of Monsel ferric subsulfate solution, and radiation intervention. Given the prognostic significance of anemia during radiation, it is hypothesized that by raising and maintaining hemoglobin level above 12 g/dl using erythropoietin may decrease secondary hypoxia and improve survival. GOG performed a prospective randomized trial comparing maintenance of a hemoglobin level at or above 12 g/dl with recombinant human erythropoietin or maintenance of a hemoglobin level at or above 10 g/dl with transfusion.45 Of eligible patients, 109 were randomized to the two arms of the trial. The trial was closed prematurely because of potential concerns for thromboembolic events (TEs).46 The rate of TEs was 4 of 52 in the chemoradiotherapy arm versus 11 of 57 in the erythropoietin arm. However, the difference in rate of TEs was not significantly different.
The questionable influence of endometrial extension on outcome is inter-related with the volume of tumor as well as the issue of parametrial extension (stage). Several retrospective reports identify endometrial stromal invasion as having a negative affect on survival, possibly because of an increase in distant metastases rather than an increased incidence of local failure after definitive irradiation.47,48
Young age at diagnosis appears to carry with it a worse prognosis.40,42,49–51 Karnofsky performance status has been identified as an independent prognostic factor of actuarial survival in the GOG analysis of 606 patients entered into three consecutive radiation therapy trials.52
Women with cervical cancer and HIV tend to present with more advanced disease compared with seronegative patients.53,54 In a report of 84 patients evaluated and treated for cervical cancer at the State University of New York, 16 patients were known to be HIV-positive. Only one of these patients presented with early stage disease, compared with 40% of the remaining 68 HIV-negative women. Of the 16, 10 suffered recurrences after a brief interval, 4 were either lost to follow-up or died shortly after therapy, and only 2 experienced long-term control. The mean CD4 count, a crude indicator of the immune status of the patient, was 360 compared with 830 for the HIV-negative group. The only two long-term survivors were patients with initial CD4 counts greater than 600. HIV status, taken in conjunction with other measures of the immunocompetence of the patient (such as frequency of opportunistic infections, CD4 count) has a profound influence on tolerance to therapy and overall survival.53
Staging and Workup
Diagnostic Workup and Staging
The current FIGO staging system has evolved during the past 60 years from its initial formation in 1929 as the League of Nations Health Organization system (Table 48-4). Various changes have been made during that interval to incorporate applicable information, such as the removal of corpus extension from staging consideration (1950) and the creation of stage IA in 1962 and its later subdivision into IA1 and IA2 (1972), and IB1 and IB2 (1998). In the current system, Stage IIA is further subdivided into stage IIA1 and IIA2 (2010).
Table 48-4 Classification of Uterine Cervix Cancer
Rights were not granted to include this table in electronic media. Please refer to the printed book.
The 5-year survival rate for patients with stage IB disease can vary from less than 20% for patients with bulky disease and both pelvic and para-aortic adenopathy to greater than 90% for those with lesions less than 2 cm in maximum diameter and no involved nodes.55 Survival rates for patients with higher staged disease also vary within each stage depending on primary tumor volume and nodal status.37,56 In the Patterns of Care report on the uterine cervix, the differentiation between IA and IB was not found to predict for either 5-year actuarial survival or pelvic control, whereas the presence of bulky disease did correlate with a higher pelvic failure rate in stage IB disease.56 In stage II disease, unilateral versus bilateral disease significantly affected both actuarial survival and pelvic control rates, a significance that persisted on multivariate analysis. In the analysis of stage III disease, the differentiation between unilateral or bilateral sidewall or lower-third vaginal involvement was highly significant in both actuarial survival and pelvic control results. The GOG findings regarding the great prognostic significance of para-aortic adenopathy and tumor volume also point out the shortcomings of the current system.40
The American Joint Committee on Cancer has devised a tumor-node-metastasis system similar to the FIGO system. The FIGO staging system is most widely used (see Table 48-4), despite its shortcomings. For practical purposes of reporting, it is imperative that the clinical staging rules be adhered to in order to ensure accurate comparisons of therapeutic interventions. The rules for clinical staging according to FIGO state that staging is to be based on careful clinical examination prior to intervention, preferably an examination under anesthesia. Once established, the stage is not to be changed by later findings or therapeutic interventions. Palpation, inspection, colposcopy, endocervical curettage, hysteroscopy, cystoscopy, proctoscopy, intravenous urography, and x-ray examination of the lungs and skeleton are recommended. Suspected involvement of the bladder or rectum must be documented by histology. Specifically excluded from the clinical staging system are the results of such tests as lymphangiography, fine-needle aspiration or biopsy of lymph node, magnetic resonance imaging (MRI), computed tomography (CT), positron emission tomography (PET), laparoscopy, and laparotomy. These tests are not allowed to influence the clinical stage for reporting purposes but may be used for treatment planning and providing important diagnostic information.
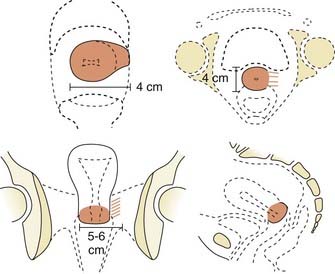
Locally, it is important to fully describe the extent of palpable disease through the use of extensive diagrams and descriptions of the three-dimensional (3-D) characteristics of the lesion (Fig. 48-4). The degree of parametrial (medial or lateral, unilateral or bilateral) or vaginal (upper two-thirds, lower one-third) extension should be clearly defined, as should the presence or absence of hydronephrosis, rectal invasion, bladder mucosal invasion, bullous edema, uterosacral ligament involvement, or extension to the pelvic sidewall (bilateral or unilateral). The use of MRI evaluation of the pelvis is not allowed by the current staging system in determining the clinical stage but has proven to be of benefit in defining the extent of disease locally as well as regionally. It also provides information that is useful in optimizing brachytherapy planning. Cystoscopy and proctosigmoidoscopy are routinely called for by the FIGO system, but in cases of early disease in which MRI shows no suspicion of local extension, these more invasive procedures may not be necessary. On the other hand, if an MRI scan raises the question of bladder or rectal involvement, endoscopic evaluation is essential to rule out pathologic involvement of these organs. A CT scan with contrast can provide information as to the presence of hydroureterosis or hydronephrosis.
Positron emission tomography (PET) has become a useful staging modality for locally advance cervical cancer. It may be an accurate noninvasive method of evaluating nodal status, endometrial extension, tumor volume, and prognosis.57–60 PET scan also may play an important role in post-therapy monitoring. Grigsby and associates showed that patients treated with radiotherapy who had a normal 3-month post therapy PET scan had a 5-year cause-specific survival of 80%.61 Another study shows PET scans as an effective way of detecting asymptomatic recurrence.62
Further routine workup should include a complete blood count, liver function tests, renal function tests, and a chest x-ray. In patients believed to be at risk for exposure to HIV, testing for antibodies to HIV should be discussed with the patient prior to the initiation of therapy. If the patient is HIV antibody–positive, the CD4 count is currently recommended as a rough indicator of the immune status and of the patient’s likelihood to be able to tolerate therapy.53 The usefulness of a bone scan is limited to patients with advanced disease with symptoms suggestive of dissemination and is not routinely obtained. In cases in which there is evidence of spread to pelvic lymph nodes on pelvic CT or MRI scan, evaluation of the abdomen to rule out higher adenopathy or liver involvement is recommended.
Blind scalene node biopsy performed in the setting of positive para-aortic lymphadenopathy has a positive rate of 0% to 35%.63 In a prospective evaluation of biopsies of nonpalpable scalene nodes in 55 patients with positive para-aortic (48) or high common iliac nodes (8), only 4 were confirmed positive (14%).64 The routine use of such biopsies is not warranted. Prior to the initiation of para-aortic radiation for patients with known retroperitoneal disease, CT scan of the chest to rule out disease missed on plain chest x-rays may be a more useful test than biopsy of clinically negative nodes.
Management Newly Diagnosed Cervical Cancer
Carcinoma In Situ and Stage IA Disease
CIS and disease with early stromal invasion isolated to buds of neoplastic cells that penetrate the basement membrane but remain immeasurable macroscopically (stage IA) have essentially a 0% incidence of involvement of the lymph nodes.65–67 In the absence of disease at the cone biopsy margins, a recurrence rate of 0% would be expected after simple hysterectomy. Conization itself represents adequate therapy in these cases, as long as the margins are definitely clear. A lesion cannot be classified as stage IA disease unless all margins of the cone biopsy are free of disease, because the entirety of the lesion may not have been identified. Alternative approaches such as laser vaporization and cryotherapy have success rates in excess of 95%, although obliteration of the margins may make it difficult to identify those patients with residual disease.65,68
The presence of LVSI or invasion to a depth greater than 3 mm is associated with a slight increase in the risk of spread to pelvic nodes or recurrence after hysterectomy. Up to 13% of patients with these findings may have lymphatic spread at time of hysterectomy (range 2%-13%),66,67






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


