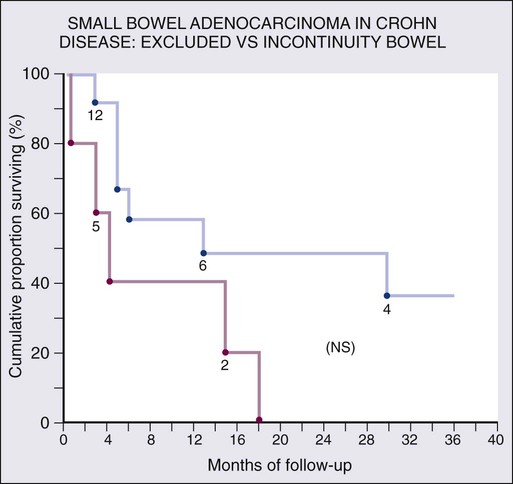
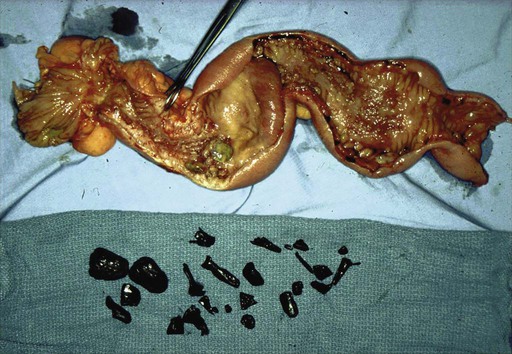
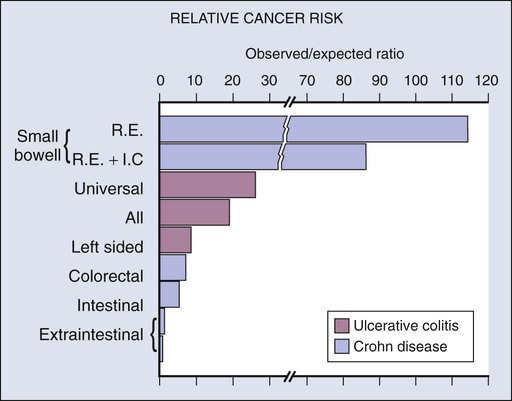
Laura Doyon, Alexander Greenstein and Adrian Greenstein • Small bowel tumors are rare, with incidence of less than 10% of new gastrointestinal cancer diagnoses and less than 1% of all new diagnosed cancers each year. • Genes involved include APC and KIT and mismatch-repair genes. • Malignant small bowel tumors consist of carcinoid (37.4%), adenocarcinoma (36.9%), lymphomas (17.3%), and gastrointestinal stromal tumors (GISTs) (8.4%). • Staging is based on the American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) staging system. Gastrointestinal (GI) lymphoma is staged with the Ann Arbor system based on lymphatic and extra lymphatic involvement above and below the diaphragm. • Primary therapy for small bowel neoplasms is surgical resection. Appropriate lymphadenectomy must be performed for adenocarcinoma and carcinoid tumors. • Chemotherapy is often used for adenocarcinoma; however, there is no clear benefit for prognosis. GISTs are treated with tyrosine kinase inhibitors. Treatment of Metastatic Disease • Surgery may be used to control complications of local symptoms such as bowel obstruction. Chemotherapeutic options are being explored that do not have a clear benefit for prognosis as of this time. • Gastrointestinal bleeding, mechanical obstruction, pain, and perforation may require palliative surgery in situations when curative resection is not possible. The use of palliative chemotherapy is also being explored. Somatostatin analogs are used in carcinoid syndrome. Small bowel cancer is rare, comprising less than 1% of new cancer diagnoses each year. The estimated incidence of new cases of small bowel malignancies in 2012 is 8,070, with 1,150 deaths. This is in contrast to the estimated new cases of colorectal cancer totaling 143,460, with 51,690 deaths. Small bowel cancer makes up less than 10% of gastrointestinal cancers each year.1 However, 17 years later, results from 2004 SEER database documented that the overall incidence of small bowel malignancies increased (from 2.1 to 9.3 per million). Carcinoid tumors have now superseded adenocarcinoma in incidence: carcinoid 37.4%, adenocarcinoma 36.9%, lymphomas 17.3%, and stromal tumors 8.4%.2 The overall increased incidence appears to be largely due to carcinoid tumors; it is unclear whether this is due to improved imaging, because most carcinoids are asymptomatic. SEER trends from 1973 to 2000 showed an increasing incidence in black men, who had roughly double the rate of incidence of both carcinoid and carcinoma compared with whites (10.6 vs. 5.6 per million people and 9.2 vs. 5.4 per million people, respectively).3 The rarity of small bowel cancer has made the study of its pathogenesis difficult. However, the etiology of small intestinal adenocarcinoma may be similar to that of colon cancer because it appears to share the adenoma-carcinoma sequence previously described in colon cancer.4 Nevertheless, although the small bowel contains 90% of the mucosa of the GI tract, it is surprising that this results in only 1% to 2% of gastrointestinal malignancies. Previous theories as to why cancer of the small bowel mucosa is so rare compared with the colon include the small bowel’s lower bacterial load and faster transit time of ingested carcinogens. The three main categories of risk factors include environmental, genetic, and chronic inflammatory factors. Familial adenomatous polyposis (FAP) is caused by an autosomal dominant mutation in the adenomatosis polyposis coli (APC) gene. In addition to the thousands of colonic polyps these patients typically develop, patients have nearly 100% cumulative lifetime risk of developing duodenal polyps that may become malignant. In fact, in postcolectomy patients, duodenal cancer as well as abdominal desmoid tumors seem to be the most important factors in long-term cancer risk.6 Hereditary nonpolyposis colon cancer (HNPCC) is a condition caused by loss of DNA mismatch repair genes and predisposes patients to increased risk of small bowel adenocarcinoma in addition to colonic carcinoma. In a series by Rodriguez-Bigas et al., 42 individuals with HNPCC developed 42 primary and 7 metachronous small bowel tumors, with 46 adenocarcinomas and 3 carcinoids. The small bowel was the first site of carcinoma in 57% of these patients.7 Lastly, Peutz-Jeghers syndrome is an autosomal dominant polyposis disorder with substantially increased relative and absolute risk of several types of cancer, including adenocarcinoma of small bowel.8 Chronic mucosal inflammation has been noted as a cause for development of adenocarcinoma and lymphoma. A series of patients with inflammatory bowel disease (IBD) at The Mount Sinai Hospital demonstrated that 67% of GI cancers associated with Crohn disease and 96% of those associated with ulcerative colitis were located in diseased bowel.9 In this series, seven cancers were found in the bypassed loops of diseased bowel, an operation seldom performed today (Fig. 76-1).10 In general, small bowel tumors are almost always discovered late because presenting symptoms are vague. Pain, often crampy, is the most common presentation, followed by nausea and vomiting, and then weight loss. Small bowel obstruction tends to occur more often in malignant cases, whereas GI bleeding is more frequent with benign tumors.11 Mean age at presentation is 65 years, with a slight predominance in men.12 The mean age in Crohn disease–related small bowel cancer is about a decade earlier.10,13 Adenocarcinoma presents most often in patients between ages 50 and 70 years, but predisposing factors such as Crohn disease may cause an earlier presentation. Prevalence is slightly increased in males. In a series of 491 patients with small bowel adenocarcinoma, the following distribution of presenting symptoms was noted: abdominal pain (43%), nausea and vomiting (16%), anemia (15%), overt GI tract bleeding (7%), jaundice (6%), weight loss (3%), other or no symptoms (9%).14 More proximal lesions present with nausea and vomiting, and distal lesions present with crampy pain and distention before the onset of vomiting. Although adenocarcinoma associated with Crohn disease tends to occur in the ileum, isolated cases of adenocarcinoma may occur in the duodenum. Diagnosis is particularly difficult in Crohn disease despite the increased incidence because of the difficulty of surveillance even with the more recent use of capsule endoscopy. The symptoms are difficult to differentiate from the symptoms of obstructing Crohn disease (Figs. 76-2 and 76-3). Physicians should consider this possibility if symptoms recur after a long period of quiescence. Pathology reports from the population-based Cancer Surveillance Program found that 50% of small bowel adenocarcinoma occurred in the duodenum, and half of those were located in the second portion specifically, despite the fact that the duodenum composes only 4% of small bowel length. Possible explanations are that bile might be carcinogenic, or that the alternating acidic and alkaline environments from gastric and pancreatic secretions may be caustic.15 Although there is a well-documented increased relative risk of developing intestinal adenocarcinoma in Crohn disease compared with the general population, it is still rare (Fig. 76-4). A 25-year history of regional ileitis only confers a cumulative risk of 2.2%.16 The authors’ experience at The Mount Sinai Hospital between 1960 and 2009 involved 48 cases of small bowel carcinoma in two series of patients with Crohn disease. The overall average time between initial diagnosis of Crohn disease to diagnosis of small bowel adenocarcinoma was 25.8 years.10,13 Because early symptoms are vague, these tumors often present at a late stage: 3% present as carcinoma in situ, 12% as stage I, 27% as stage II, 26% as stage III, and 32% as stage IV.17 As with colorectal adenocarcinoma, the primary therapy of localized small bowel adenocarcinoma is radical segmental resection including associated mesentery and lymph nodes. Adequate nodal resection provides vital information for staging as well as clearance of early lymph node metastases. For tumors of the duodenum, traditionally pancreaticoduodenectomy has been performed; however, there is some suggestion that segmental duodenal resection may be performed especially for more distal lesions.18 Tumors of the terminal ileum require an ileocolic resection.
Cancer of the Small Bowel
Epidemiology
Pathogenesis and Risk Factors
Genetic Factors
Chronic Inflammation
Clinical Presentation
Malignant Tumors of the Small Bowel
Adenocarcinoma
Symptomatic Presentation

Surgical Management
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oncohema Key
Fastest Oncology & Hematology Insight Engine