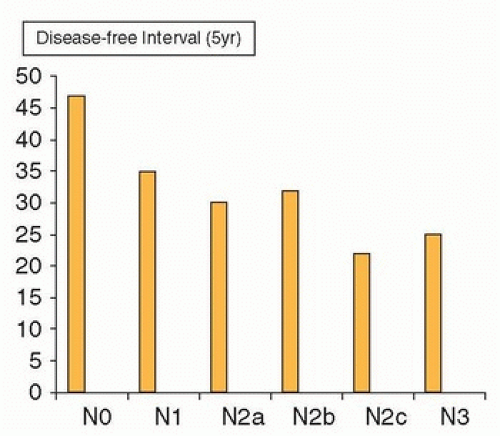
 Figure 18.1. Impact of the extent of neck metastases (N stage) on prognosis. Disease-free interval according to TNM staging. (Modified from Kowalski LP, Bagietto R Lara JR, et al. Prognostic significance of the distribution of neck node metastasis from oral carcinoma. Head Neck. 2000;22:207-214.) |
the SCM, also known as Erb point (Fig. 18.4).4 The mean distance between the Erb point and the SAN is 10.7 mm, SD ± 6.3. It then runs through the posterior triangle of the neck and crosses the anterior border of the trapezius muscle. The mean distance between this point and the clavicle is 51.3 mm, SD ± 17.4 Two anatomic characteristics of this portion of the nerve are relevant to avoid injuring it in the course of a neck dissection. First, the SAN is located rather superficially as it courses through the middle and low posterior triangle of the neck, and it can be easily injured while elevating the skin flaps in the posterior neck. Second, the nerve does not enter the trapezius muscle at the anterior border of it but courses along the deep surface of the muscle in close relationship with the transverse cervical vessels. Therefore, isolating the nerve to the level of the anterior border of the trapezius does not ensure its preservation during surgical dissection below this point, particularly in a bloody operative field.
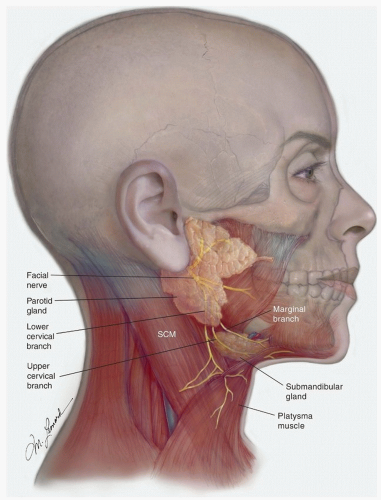 Figure 18.2. Anatomy of the inferior division of the facial nerve: 1. Marginal mandibular branch; 2. Upper cervical branch; 3. Lower cervical branch. |
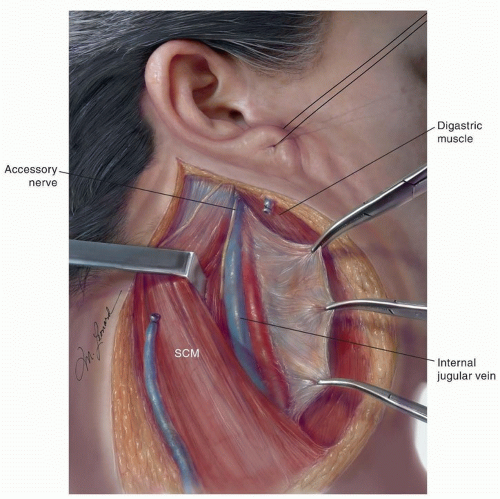 Figure 18.3. The SAN in its most common position in the superior aspect of the right neck: lateral and slightly posterior to the IJV. |
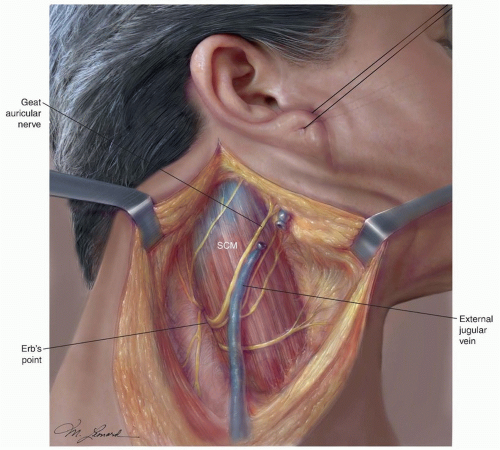 Figure 18.4. The spinal accessory in the posterior triangle of the neck. 1. Erb point; 2. The SAN is usually located about 1 cm above Erb point. |
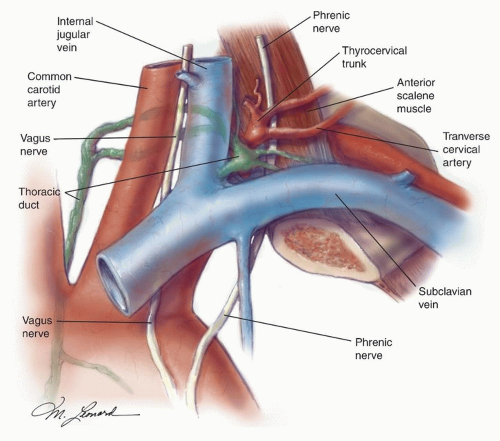 Figure 18.5. Anatomic relations of the thoracic duct. 1. Vagus nerve; 2. Common carotid artery; 3. Internal jugular vein; 4. Phrenic nerve; 5. Thoracic duct draining into the subclavian vein; 6. Transverse cervical artery. |
nerve. It then opens into the IJV, the subclavian vein, or near the angle formed by the junction of these two vessels. The duct is anterior and medial to the thyrocervical trunk and the transverse cervical artery. To prevent a chyle leak, the surgeon also must remember that the thoracic duct may be multiple in its superior aspect and that at the base of the neck it usually receives a jugular, a subclavian, and other minor lymphatic trunks, which must be ligated or clipped individually.
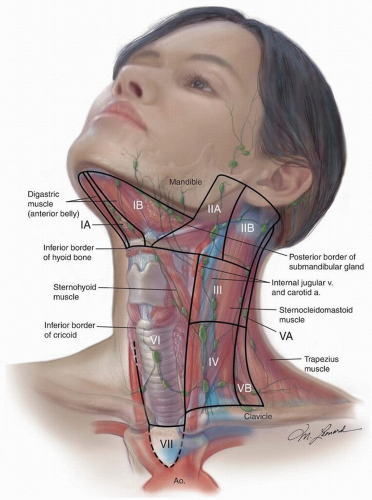 Figure 18.6. The lymph node regions/“levels” of the neck. |
lymph nodes of the neck that are removed and secondarily the anatomic structures that may be preserved, such as the SAN and the IJV. Analyzing neck dissections from these two points of view, there are essentially four anatomic types of neck dissections: radical, modified radical, selective, and extended. Recently, clinicians from around the world have proposed a nomenclature for neck dissection, which, if recognized internationally, would be “logical, unambiguous, precise, and easy to remember.”10
Table 18.1 Classification of Neck Dissections | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
“ND” to represent neck dissection, which is prefaced by either “L” or “R” for side. If bilateral, both sides must be classified independently.
The levels and sublevels of lymph nodes removed designated by Roman numerals I through VII in ascending order. For levels that contain sublevels (I, II, and V), listing of the level without a sublevel indicates that the entire level (both A and B) was excised.
The nonlymphatic structures removed designated by their internationally recognized initials, that is, SCM for sternocleidomastoid muscle and IJV for internal jugular vein.
Table 18.2 Nodal Size and Presence of Histologic Metastases | |||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||
It appears that lymphoscintigraphy in cancers of the floor of the mouth is not as helpful in identifying the SLN; this is most likely due to the “shine-through” effect of the radioactivity at the primary, which obscures the lymph nodes in level I, the primary echelons of lymphatic drainage for the floor of the mouth and inferior Alvestar ridge. Obviously, this limits the utility of SLNB in patients with tumors in these locations.
Table 18.3 Oral Cavity Squamous Cell Carcinoma Incidence of Lymph Node Metastases by Stage | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||
a rate of cervical lymph node metastasis significantly higher than cancers with a depth of invasion <3.25 mm (p < 0.05). Expression of epidermal growth factor (EGFR) is another potentially useful biologic marker. A significant correlation between expression of EGFR and the risk of lymph node metastases was observed by Maurizi et al.,57 in a study of 140 cases of carcinoma of the larynx. In a similar study, Almadori et al.58 observed that the 5-year lymph node metastasis-free survival was 66% for patients with EGFR-negative larynx cancers compared with 15% for patients with EGFR-positive tumors.
Table 18.4 Squamous Cell Carcinoma of the Oropharynx: Incidence of Lymph Node Metastases by Stage (Based on Histopathology of Neck Dissection Specimens) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||
Table 18.5 Squamous Cell Carcinoma of the Oropharynx: Incidence of Bilateral Nodal Metastases59 | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
Whether to perform a neck dissection or to observe the neck and intervene only if and when lymph node metastases become apparent.
What type of neck dissection is appropriate.
Patterns of lymph node metastases: Anatomic, pathologic, and clinical investigations41,64,65,66,67,68,69,70,71,72,73,74 as well as recent prospective studies75,76 have demonstrated that cervical lymph node metastases occur in predictable patterns in patients with SCCs of the head and neck.
The lymph node groups most frequently involved in patients with carcinomas of the oral cavity are the nodes in levels I and II. The nodes in level Ia are frequently involved in patients with carcinoma of the floor of the mouth and anterior oral tongue. These cancers frequently metastasize to both sides of the neck, and they can skip levels I and II, metastasizing first to the nodes in level III. In a retrospective study of 1,119 RNDs, Shah71 found that cancers of the oral cavity metastasized most frequently to the neck nodes in levels I, II, and III, whereas carcinomas of the oropharynx, hypopharynx, and larynx involved the nodes in levels II, III, and IV.
It has been demonstrated that in the absence of metastases to the first-echelon nodes, cancers of the oral cavity and oropharynx rarely involve the nodes in level IV and level V. The nodes in level V are not commonly involved, regardless of the site of the primary tumor and whether in the presence or absence of metastases in the jugular nodes,77 conceivably because there is no retrograde flow from the jugular nodes into the spinal accessory nodes.
Similarly, in a prospective analysis of the prevalence and distribution of histologic lymph node metastases in 100 consecutive neck dissections done as part of the initial treatment of laryngeal and hypopharyngeal cancer, Buckley and MacLennan76 found that all metastases in N0 and N1 cases were confined to levels II, III, IV, and VI. Metastases to levels I and V were infrequent, even in N+ disease, and occurred only in cases with N2c and N3 disease. These results support the use of dissection of node levels II to IV for N0 and selected N+ cases with laryngeal and hypopharyngeal cancer.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree