44 Cancer of the Bladder
Epidemiology and Etiology
Bladder cancer is estimated to have an annual incidence in the United States of 68,810 cases, accounting for 5% of all newly diagnosed cancers. Approximately 14,100 people per year will die of this disease, accounting for 2.5% of all cancer-related mortality in the United States and 3% of all cancer deaths in men.1 The incidence of bladder cancer varies considerably among countries; the highest incidence rates are in Western countries. At diagnosis, approximately 75% of patients have localized disease only, 20% have regional disease, and 5% present with distant metastases. Two thirds of all bladder cancer diagnoses occur among persons 65 years of age or older. The male/female ratio is 3 : 1. In the United States, the risk for white men is approximately twice that for African-American or Hispanic men.2 From the early 1970s to 2004 the incidence of this cancer rose slightly while mortality fell. This phenomenon is likely attributable to the increased detection of localized lesions and improved therapies.3
Cigarette smoking is the single most significant known cause of bladder cancer, as demonstrated by both cohort and case-control studies.3–8 The risk of bladder cancer appears to be related to the number of pack-years and, as such, an individual’s risk of bladder cancer declines if smoking is ceased.9 It is estimated that 50% of bladder cancers diagnosed in the United States can be linked to a smoking history.10 In a case-controlled study of more than 1500 patients with bladder cancer and a large control group matched for age, sex, and race, there was a statistically higher risk of bladder cancer observed in female smokers compared with male smokers with similar smoking habits.11 In addition, younger age at initiation of tobacco use correlates to a higher risk of developing bladder cancer.12 It appears that the relationship of smoking to bladder cancer development stems from exposure to selected arylamines. Studies have demonstrated that smokers have higher levels of 3- and 4-aminobiphenyl hemoglobin adducts, which are increased 10-fold and 3-fold, respectively, compared with nonsmokers.11 Cytogenetic analyses indicate a direct relationship between smoking and suppressor gene p53 nuclear overexpression.13
Exposure to industrial chemicals and high rates of bladder cancer in specific occupations have been a major focus of epidemiologic investigation. Individuals in contact with chemicals necessary for the production of dyes, rubber, plastics, and synthetic materials are at increased risk for development of bladder cancer.3,13–17 Dye workers may be particularly at risk owing to exposure to aromatic amines, specifically 2-naphthylamine and benzidine, which have been shown to be bladder carcinogens.18 One study demonstrated an additive effect for bladder cancer development among smokers who use hair dyes.19 There have been recent changes in hair dye formulations that appear to have decreased this risk.20 Two recent meta-analyses did not demonstrate a link to personal hair dye users and the subsequent development of bladder cancer.21,22 Rubber workers are also exposed to 2-naphthylamine, and benzidine is found in paints.3 Dry cleaners may have an increased risk of bladder cancer from exposure to organic solvents, including perchloroethylene.23
Schistosoma haematobium is presumed to be the primary cause of endemic squamous cell carcinoma common in Egypt.24 This form of bladder cancer is recognized to occur in patients 10 to 20 years younger than patients with typical cases of transitional cell carcinoma diagnosed in the United States.25 It has been hypothesized that the parasite may induce an inflammatory response that includes the release of reactive oxygen radicals, which results in genetic damage, leading to carcinogenesis.26 Patients with chronic urinary tract infections or with the need to frequently self-catheterize after spinal cord injury are also predisposed to squamous cell carcinomas.27–29 Mechanisms proposed include obstructive uropathy with recurrent bacterial superinfections leading to urine acidification, nitrosamine production, and bacteria-induced oxidative damage.30
Patients with a history of upper tract urothelial cancer are at high risk for the subsequent development of synchronous or metachronous cancers of the urinary bladder as well as contralateral upper urinary tract malignancies. The incidence of developing a bladder cancer is 20% to 50% regardless of the treatment modality and typically occurs within the first 2 years after treatment of the upper tract; however, lifelong surveillance is necessary in these patients.31
The role of diet in the predisposition for, or reduction of risk of, developing bladder cancer remains unclear. There have been conflicting data about the role of coffee consumption and an association with bladder cancer development. A summary of 35 case-control studies of the causal role of coffee showed no evidence of a relationship between the beverage and the development of bladder cancer.32,33 On the other hand, a recent meta-analysis for urinary tract cancers estimated a 20% increase of bladder cancers among coffee drinkers irrespective of dose or duration of consumption.34 It is now believed that there is no relationship between artificial sweeteners and the development of bladder cancer.35 Some studies have shown a minimal protective effect with vitamin A, fruits, and vegetables.36,37 People who drink fresh well water were found to have lower rates of bladder cancer than those drinking chlorinated municipal water.38 This may be related to trihalomethanes, by-products of chlorine or bromine disinfection processes, and currently most governments place restrictions on these chemicals. A higher incidence of bladder cancer has been noted in agricultural areas where fertilizers seep into water supplies, raising the level of nitrates in drinking water.39
Iatrogenic causes of bladder cancer include radiation exposure, chronic phenacetin usage, and administration of cyclophosphamide.3 Several reports have noted an increase in bladder cancer in patients who received pelvic radiation for cervical, prostate, and testicular cancers40–42; however, other studies have not established a clear causative relationship.43,44 Patients with rheumatoid arthritis were shown to have an increased rate of bladder cancer for as long as 17 years after taking oral cyclophosphamide.45
A genetic predisposition to bladder cancer in certain families has been described. It is likely that there is an interaction between hereditary predisposition of oncogenes and tumor suppressor genes that are amplified or deleted because of environmental stimuli.3 Acetylation of aromatic amines, an important mechanism of detoxification of these compounds, may be interrupted in individuals with mutations of the N-acetyltransferase genes, particularly NAT2. These “slow acetylators” have been reported to have an increased risk of bladder cancer, particularly in individuals exposed to aromatic amines and with a higher relative risk compared with “rapid acetylators” (i.e., individuals without NAT2 mutations).46 The interplay between environment and genetic predisposition is also exemplified by the reduction of glutathione S-transferase activity with the loss of the GSTM1 gene. The glutathione enzyme appears to play a role in modulating the carcinogenic effects of tobacco smoke.47,48
Cytogenetics
Scientific inquiry has concentrated on the molecular biology and cytogenetics of bladder cancer, with the expectation that insight into the natural history of the disease will translate into clinical advances. An attempt is under way to define independent prognostic factors that predict which of two similar superficial lesions is destined to relapse as muscle-invasive disease. Flow cytometry has shown that lesions with an increased chromosome number and aneuploidy were associated with higher-grade tumors destined to be invasive.49–51 One study showed that the percentages of hyperdiploid cells for chromosomes 7, 11, and 17 were predictive of grade and stage.52 Other studies have shown that FGFR3 mutation is strongly associated with low tumor grade and low risk of progression to more advanced bladder cancer.53 A model of an orderly progression of alteration in genetic material involving oncogenes and tumor suppressor genes is being elucidated.54
An early occurrence that may be critical in distinguishing Tis and T1 from normal bladder epithelium and the less aggressive papillary tumors (Ta) appears to involve loss of a tumor suppressor gene on chromosome 9.54–57 Progression to muscle-invasive disease appears to require loss of the tumor suppressor gene p53 on chromosome 17, shown to be present in 65% of Tis compared with 3% of Ta tumors.58 Other intermediate events in the progression to invasive disease likely involve deletions in 5q, 3p, and 17p, which are not present in Ta lesions.59,60 No single oncogene has been found in the majority of tumors, although c-erb B2, H-ras, c-src, and c-jun have been expressed and likely play a role in the intermediate progression to muscle-invasive lesions.61–63 Late events may involve loss of suppressor genes on 11p, 6q, 13q, and 18q.48,54,64 In particular, the loss of the retinoblastoma gene on chromosome 13 likely has a role in bladder cancer similar to its role in other malignancies.65,66 Investigators have also suggested additional loci of tumor-suppressor genes, including 4p, 8p, 14q, and 12q.67,68 Others have recently demonstrated a strong association with 6p+ and high tumor cell proliferation rate, which was noted to be an independent variable in addition to grade and tumor stage.69
A prognostic factor for transitional cell carcinoma confined to the bladder independent of grade, stage, and lymph node status is the accumulation of the p53 protein in the nucleus. With mutation of the wild-type p53, the protein product has a longer half-life and can be detected by immunohistochemistry.70 After radical cystectomy, patients with stages pT1, pT2, and pT3a who had p53 detected by immunohistochemistry had a shorter relapse-free and overall survival.71 Similarly, an analysis of p53 nuclear overexpression in 33 patients with carcinoma in situ (CIS) showed disease progression in 13 of 15 p53-positive patients compared with 3 of 18 p53-negative patients.72 The potential clinical implications of using the p53 status as a marker are far reaching and include the selection of lower-risk patients for bladder conservation and patients with early-stage disease who may benefit from adjuvant radiotherapy or chemotherapy.73–77
Anatomy
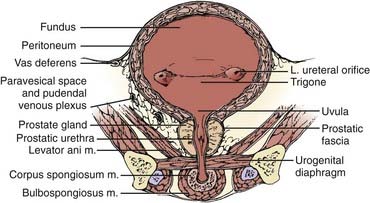
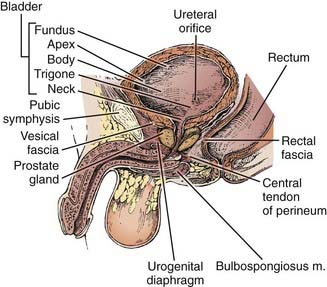
Both for the radiation oncologist and for the surgeon, the relationship between the bladder and neighboring structures is critical in treatment planning. The bladder functions as a muscular reservoir and is anatomically divided into a fundus, apex, body, trigone, and neck. Empty, the bladder is confined to the true pelvis. As the organ fills, it expands anterosuperiorly into the abdominal cavity. The fundus or base faces posteriorly and in the male is separated from the rectum superiorly by the rectovesical pouch and inferiorly by the seminal vesicles (Fig. 44-1 and Fig. 44-2). In the female, the bladder faces the uterus and the anterior vaginal wall. The neck is located 3 to 4 cm behind the symphysis pubis. This lowest and most fixed part of the bladder is pierced by the urethra and in the male approximates the prostate. A remnant of the median umbilical ligament called the urachus links the apex of the bladder (which lies posterior to the cranial section of the symphysis pubis) to the umbilicus. The superior surface of the bladder is covered by peritoneum and may approximate the sigmoid colon or ileum and the uterus in the female. Fascia forms the pubovesical ligaments that suspend the bladder between the pubic bones, anterior abdominal wall, and pelvic side walls. An empty bladder is characterized by a mucosa with folds except for a smooth triangular region called the trigone. The superior border of the trigone is characterized by its appearance as a pale band on cystoscopy and is called the interureteral crest. This band separates the ureteral openings. At the trigonal apex is the internal urethral orifice completing the triangle.78
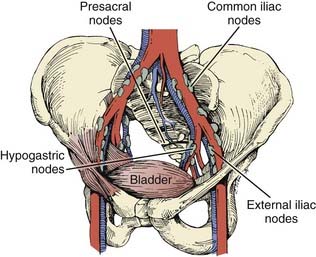
The arterial supply to the bladder arises from the anterior division of the hypogastric artery. Branches from the obturator and inferior gluteal arteries contribute to the rich vascular supply. In the female, additional vessels include the uterine and vaginal arteries. An important venous plexus exists between the bladder wall and the adventitial layer that drains into the hypogastric veins.78 Lymphatics from the mucosa and muscular layer drain to the surface of the bladder and form three collecting ducts at the trigone, anterior, and posterior walls. The trigone collecting duct drains into the external iliac nodes (Fig. 44-3). Hypogastric and common iliac lymph nodes are the destination of lymph collected in the anterior and posterior ducts. Some of the lymph also flows through the route of the anterior bladder wall collecting ducts to external iliac nodes.79
Innervation of the bladder can be divided into a parasympathetic nerve supply arising from S2-4 and a sympathetic supply that originates mainly in T11-12 and L1-2. Sympathetic nerves are found primarily in the trigone, and in the male these nerves stimulate closure of the bladder neck sphincter to prevent reflux ejaculation. Parasympathetic nerves play a large role in detrusor muscle contraction. A small group of autonomic nerves can be found scattered in the bladder wall. The adult male bladder has a normal capacity of 120 to 320 ml, with pain due to stretch sensations mediated by parasympathetic nerve fibers when distention beyond 500 ml occurs.78,80
Several anatomic variations are important with respect to a predilection to develop bladder cancer. One such variation is the persistence of a patent urachal remnant. The urachus is an embryologic canal connecting the urinary bladder of the fetus with the allantois, a structure that contributes to the formation of the umbilical cord. The lumen of the urachus is normally obliterated during embryonic development, transforming the urachus into a solid cord; however, in some children this closure fails to occur and remnants can take the form of a cyst, sinus, diverticulum, or patent urachus.81 Urachal adenocarcinoma can arise in these retained remnants. The location of these tumors are typically midline, either anteriorly or in the dome, and although often discrete, can form a large mass on the anterior abdominal wall. Urachal adenocarcimona is rare and accounts for approximately 0.35% to 0.7% of all bladder cancers.82 Extroversion of the bladder is one of the most common congenital bladder anomalies leading to a portion of the bladder, typically the mucosal surface of the fundus, protruding from the abdominal wall surface. This defect is also associated with epispadias and pelvic bone development abnormalities, and predisposes patients to bladder cancers of variable histologic anatomies.83 Adults with a history of exstrophy have a 694-fold increase in the risk of bladder cancer by the age of 40 years. Etiologic factors remain unclear, but may be related to resconstructive techniques.84 Bladder tumors are often multifocal, reflecting a “field cancerization” defect. Of the tumors that have a subsite listed at diagnosis, the majority occur on the bladder walls. The lateral walls account for 40% of malignancies, with posterior involvement of 11% and anterior involvement of 3%. As many as 17% of tumors are known to arise adjacent to the ureteral orifice, whereas the trigone, dome, and neck account for 13%, 9%, and 7%, respectively, of sites from which the cancers arise.3
Pathologic Findings
Transitional cell carcinomas account for approximately 93% of all bladder cancers in the United States.3 Pattern of tumor growth can be either papillary or flat. Papillary lesions can be either benign (i.e., inverted papilloma) or malignant. Flat lesions can be either dysplasia, CIS, or invasive cancer. In 1998, the World Heath Organization and the International Society of Urologic Pathologists published a consensus classification for urothelial malignancies that has been accepted as the standard classification schema.85 According to this schema, urothelial malignancies are classified as either low- or high-grade depending on the degree of anaplasia and architectural features. The vast majority of invasive cancers are high-grade. Noninvasive lesions are either flat or papillary.
CIS on cystoscopy often appears as multiple, flat, erythematous patches without a gross structural component. Histologic examination reveals an increase in the number of cell layers, lack of cohesion between cells that results in shedding into the urine, disordered architecture, and an increased number of mitotic figures. The basement membrane confines the tumor to the mucosa. CIS associated with an invasive tumor has been associated with a worse prognosis. Papillary lesions have exophytic stalks protruding into the lumen of the bladder. Invasive lesions show involvement of the muscularis propria layer and are often palpable on examination.86,87 The predominant histologic findings associated with invasive carcinomas are transitional cell or urothelial carcinomas. Transitional cell carcinomas often contain squamous or glandular components and are classified as transitional tumors with a natural history similar to those of pure histology. Immunohistochemical analysis of microvessel density has been shown to be an independent prognostic indicator demonstrating a relationship between tumor angiogenesis, nodal metastasis, and survival.88,89
Pure squamous cell carcinomas comprise 5% to 8% of primary bladder malignancies in the United States and Europe; however, in Egypt and other areas endemic with Schistosoma haematobium, squamous cell tumors are the predominant histologic finding. Most squamous cell carcinomas are bulky, polypoid, solid masses and often present at an advanced stage. Necrotic material and keratin debris on the surface is typical. Pure adenocarcinomas account for 1% to 2% of bladder tumors. Most often, these tumors are derived from the urothelium of the bladder (“nonurachal adenocarcinoma”) and less frequently from a urachal remnant (“urachal adenocarcinoma”). They predominantly arise in the base of the bladder or trigone, but may arise at any location.87,90 A variety of rare histologic findings account for less than 2% of all primary bladder cancers. Extrapulmonary small cell carcinoma can occasionally originate in the bladder and, because of its aggressive and high metastatic potential, it is often treated with chemotherapy generally used for small cell carcinomas of the lung in addition to local therapy.91 These patients may be younger (median 40-60 years); however, similar to other histologic findings, small cell carcinoma of the bladder is associated with smoking.92 Because of the rarity of this finding, there are no prospective trials designed to define the best management of these patients. Poor long-term survival has been seen with single-modality therapy; therefore, combined-modality regimens are typically used.92 Rhabdomyosarcoma of the bladder occurs in children but rarely presents in adults.93 Other rare histologic findings include lymphoma, leiomyosarcoma, melanoma, and primary bladder pheochromocytoma.94–97 In addition, adenocarcinomas can metastasize to the bladder from the colon, rectum, endometrium, prostate, ovary, breast, and lung.98
Clinical Presentation and Routes of Spread
Gross or microscopic hematuria is a presenting sign in 75% of patients with bladder cancer. Approximately 25% of bladder cancer patients present with symptoms of bladder irritation (i.e., urinary frequency, urgency, dysuria), especially patients with CIS. Typically, symptoms are intermittent and diagnosis is often delayed as these may be similar to benign disorders such as cystitis, prostatitis, or bladder stones. Advanced tumors may present as pelvic pain, ureteral obstruction, hydronephrosis, or rectal obstruction.99,100
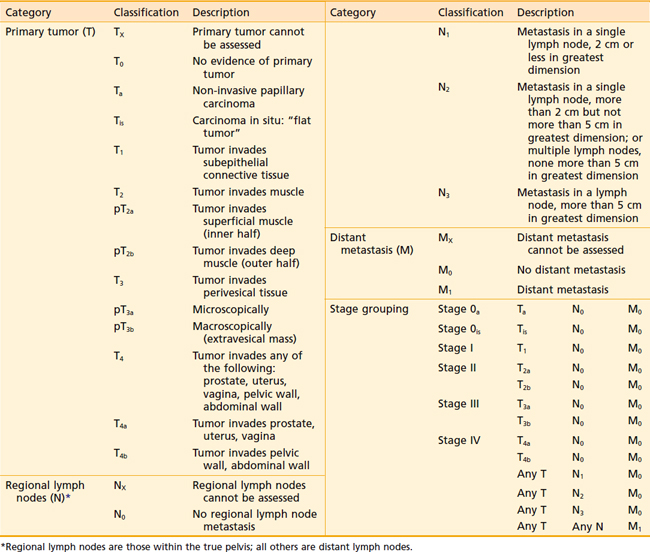
The regional lymph nodes at risk as defined by the current American Joint Committee on Cancer (AJCC) 2002 staging system are those in the true pelvis below the bifurcation of the common iliac arteries. These lymph nodes include the hypogastric, obturator, internal and external iliac, perivesical, pelvic, sacral, and presacral chains. Staging depends on the size and number of involved nodes, but not on whether they are unilateral or ipsilateral (Table 44-1). Spread to the common iliac nodes is considered a manifestation of distant metastases and not regional disease.101 Recent surgical series, however, have demonstrated long-term disease control in patients undergoing cystectomy with positive lymph nodes from extended lymph node dissections including the periaortic, common iliac, and presacral chains (see Surgical Treatment of Muscle-Invasive Bladder Cancer).102,103 The extent of nodal dissection currently remains controversial and the staging system has not yet been altered. Skinner and colleagues104 correlated the depth of bladder wall invasion to involvement of lymph nodes. In their study, 5% of patients with pT1, 30% with pT2, 31% with pT3a, 64% with pT3b, and 50% with pT4 disease had nodal metastases. The most common sites of distant metastatic disease are the lung, bone, and liver.
Diagnostic and Staging Studies
The initial formulation of an organized staging system reproducible in predicting survival dates back to the work of Jewett and Strong in the 1940s. Primary bladder tumors were classified as stage A when involvement was limited to the submucosa, as stage B when tumor penetrated into the muscularis, and as stage C when there was evidence of perivesical fat involvement. Stage A tumors had no evidence of metastases compared with 13% of stage B tumors and 74% of stage C tumors. In 1951, Jewett proposed a division of stage B into B1 and B2 to correspond with superficial and deep muscle penetration. The following year, Marshall added a stage 0 to include tumors not infiltrating the lamina propria and stage D for metastatic disease.105
The current tumor-node-metastasis (TNM) staging system standardized by the AJCC and the TNM Committee of the International Union Against Cancer continues to reflect the importance of depth of bladder wall invasion. The T stands for depth of tumor in relation to the mucosa, muscularis, and the perivesical fat. Regional nodes include those of the true pelvis, whereas M disease involves nodes above the bifurcation of the common iliac arteries or distant visceral metastasis.101
The current TNM staging system (see Table 44-1) recognizes that Ta papillary growths convey a significantly better prognosis than Tis (CIS) or T1 lesions. Also recognized is that either microscopic (T3a) or gross involvement (T3b) of perivesical fat is more important than the distinction between superficial (T2a) or deep muscle invasion (T2b). Stage T4 includes locally advanced tumors that invade the prostate, uterus, or vagina (T4a) or directly adhere to the pelvic or abdominal wall (T4b).101
The presence of gross hematuria in a patient older than 40 should raise suspicion for urothelial carcinoma until proven otherwise, particularly in a patient with known risk factors. Approximately 20% of all patients presenting with gross hematuria and 5% to 10% of all patients with microscopic hematuria will ultimately be diagnosed with bladder cancer.106,107 A history and physical examination should be followed by a urinalysis with urine cytologic study to detect the presence of suspicous cells. A cystoscopic examination includes documentation on a bladder diagram of tumor location, number of lesions, pattern of growth, and tumor size. A bimanual examination should be performed before and after endoscopic resection and is an important part of clinical staging. A mobile bladder mass indicates a T3 tumor, whereas a fixed mass suggests T4 disease. A transurethral resection of a bladder tumor (TURBT) is diagnostic and often therapeutic in superficial lesions. Muscle must be seen by the pathologist in a biopsy or transurethral resection for it to be an adequate indicator of prognosis. Biopsy specimens of surrounding and apparently unaffected areas, including the prostatic urethra, are taken because CIS may be visibly indistinguishable from normal mucosa. Persistence of a palpable mass on examination under anesthesia after TURBT identifies a poor prognostic group, usually with T3b disease.108 Patients with muscle-invasive disease require a screening workup for metastatic disease that includes chest imaging by either computed tomography (CT) or plain films as well as pelvic imaging to identify nodal involvement using CT or magnetic resonance imaging (MRI) of the pelvis. Imaging should include the abdomen if there is pelvic nodal disease or abnormal results of liver biochemistry studies. The upper urinary tract should be imaged with intravenous urography or contrast CT urogram to rule out synchronous upper tract lesions. In patients with invasive or locally advanced disease or in patients with elevation of the serum alkaline phosphatase level or bone pain, a bone scan should be performed to rule out metastases.108,109
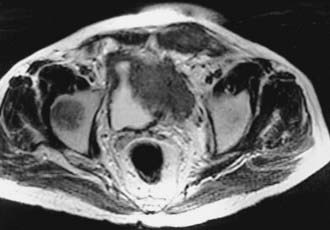
Imaging with CT or MRI has an important role in defining the extent of disease for locally advanced bladder lesions. Mural and mucosal lesions are distinguishable from perivesical fat and urine, allowing visualization of papillary and extravesical lesions (Fig. 44-4). Important diagnostic information that can be demonstrated with CT is the presence of gross perivesical extension or lymphadenopathy.110 Understaging of local disease, however, remains an important problem with clinical staging evaluations. Although not always as available as CT, MRI may be more accurate in determining the T stage of bladder tumors.111 MRI has many advantages over other modalities for detecting and staging bladder neoplasms because of its intrinsic high soft tissue contrast, direct multiplanar imaging capabilities, and the availability of a non-nephrotoxic, renally excreted contrast agent. Tachibana and coworkers112 correlated imaging with histologic staging for 57 bladder tumors. The sensitivity and specificity for differentiating superficial and invasive tumor were 96% and 83% for gadolinium-enhanced MRI, 96% and 58% for CT, and 88% and 67% for transurethral ultrasonography. The contrast between tumor and fat is critical for evaluating locally advanced lesions and is best detected on T1-weighted images. It is important to recognize in the post-treatment management of the patient that changes in signal intensity of normal bladder wall 3 to 4 months after irradiation limit the usefulness of MRI in detecting tumor recurrences.113 Reports indicate improved accuracy in staging muscle-invasive tumors when MRI is performed with gadolinium-enhanced images. Tanimoto and associates114 showed that for 86 tumors, MRI with gadolinium enhancement had a staging accuracy of 85%, in comparison with 55% for CT scan and 58% for conventional MRI. Detection of superficial lesions was improved and there was a decrease in the overstaging of T1 tumors. Sensitivity and specificity of MRI for staging bladder tumors have been improved with the advent of imaging with oblique planes, smaller pixel size, and three-dimensional (3-D) technology. Applying 3-D technology to MRI was associated with improved accuracy of local staging from 78% to 93% and nodal staging from 86% to 93%.113,115,116 The detection of nodal involvement with clinical staging has obvious treatment-planning implications for the radiation oncologist. One report from the Christie Hospital in the United Kingdom demonstrated that preradiotherapy staging with MRI was helpful in providing more anatomic detail and clarifying the extent of disease. In that series, 39 of 71 patients with clinical T2a tumors were upstaged. Among the 27 patients in that series upstaged to T3b, this group experienced a significantly worse local control and overall survival outcomes. A multivariate analysis demonstrated that, among other variables, tumor stage based on MRI was a significant factor predicting for treatment failure and overall survival.117 MRI may be particularly helpful in the evaluation of direct prostatic extension of tumor (T4a).118
The role of fluorodeoxyglucose (FDG)–positron emission tomography (PET) remains controversial in patients with superficial and locally advanced bladder cancer. The presence of radiotracer in the urine makes interpretation of early stage disease problematic. For the early detection of locally advanced bladder cancer with lymph node involvement, FDG-PET shows promise. FDG-PET imaging prior to cystectomy had a sensitivity of 67% and a specificity of 86% for detection of lymph node metastases, which compares favorably with conventional CT.119 FDG-PET appears able to detect metastatic lesions with high frequency as well.120 The full role of FDG-PET and other PET technology has yet to be realized in bladder cancer.
Pathologic staging requires either a partial or total cystectomy and lymph node dissection. Suspected metastatic disease on imaging studies can often be confirmed by CT-guided biopsies. Staging error between clinical and pathologic stages has been shown to be as high as 50%.101 Survival is lower for each stage when grouped clinically as opposed to pathologically. It is for this reason that comparing outcomes of radiotherapy series based on clinical staging with surgical series based on pathologic staging is fraught with difficulties. Nevertheless, with both modalities, survival decreases with increasing stage. This provides the clinician with the necessary prognostic information to formulate a treatment approach.108
Identification of prognostic factors allows the clinician to select those patients who would potentially benefit from bladder conservation approaches or, conversely, patients better managed with upfront radical cystectomy. Advanced-stage disease has been shown to be an accurate predictor for a high risk of developing early distant metastases.109 In addition to the depth of invasion and the presence or absence of nodal involvement reflected in the stage, other prognostic variables have been defined. Low-grade and papillary growth have been shown to represent good prognostic indicators for survival.121 Tumors characterized as larger than 5 cm, with associated CIS, with evidence of vascular invasion, and with failure to obtain a complete response to chemoradiation have been shown to have a poor outcome and these patients may be better suited for cystectomy.122 The presence or absence of hydronephrosis has also been correlated with prognosis in both cystectomy and radiation therapy series.123,124 Researchers have indicated that a tumor with a high degree of angiogenesis may have a poorer prognosis.89 It is likely that in the future prognostic factors will be increasingly identified at the cytogenetic level.
Treatment of Superficial Bladder Carcinoma
Three fourths of bladder carcinomas present as Ta, T1, or Tis superficial lesions that do not extend deeper than the lamina propria. Although the majority of such tumors are controlled by transurethral resection, an estimated 40% to 80% will recur within 6 to 12 months and 10% to 25% will progress to muscle-invasive disease. Prognostic factors for recurrence include grade, depth of penetration, multifocality, and presence of CIS. The management of superficial bladder carcinoma involves TURBT and, in many cases, adjuvant therapy to prevent recurrence and potential development of muscle-invasive disease.99,125,126
Ta papillary tumors typically present as low-grade lesions that frequently recur multiple times prior to progressing to invasive tumors. Low-grade Ta papillary lesions without multifocality and without associated CIS can be treated with a diagnostic and therapeutic resection using a resectoscope, followed by close monitoring and repeat cystoscopies. Muscle must be seen in this specimen before ruling out invasive disease and biopsies of apparently uninvolved urothelium should be obtained to rule out occult Tis. Approximately 5% to 30% of patients will ultimately progress to a higher-grade lesion or require more aggressive therapy.127,128 For patients with persistent tumor cells on urine cytology after TURBT, multifocal lesions, grades II or III histologic findings, or evidence of CIS, adjuvant intravesical therapy is indicated. If all visualized superficial lesions are not excised, there is also a need for further therapy. Adjuvant therapy is given in the form of intravesical administration of immunotherapy or chemotherapy. Bacille Calmette-Guérin (BCG) is administered adjuvantly weekly for 6 weeks. BCG, a live attenuated form of Mycobacterium bovis, has an unknown exact mechanism of action; however, it triggers an immune-response cascade including mononuclear cells and cytokines such as interleukin (IL)-1, IL-2, IL-6, IL-8, interferon-γ, and tumor necrosis factor-α. In addition, a direct tumor-cell suppression may be involved. The chemotherapeutic agents of greatest known efficacy are mitomycin C, doxorubicin, and thiotepa. These three agents have all demonstrated efficacy in the reduction of disease recurrence.126 Thiotepa causes the most systemic toxicity, including myelosuppression in 20% of patients, owing to its low molecular weight, which allows absorption. Doxorubicin creates the greatest local reaction, which may predispose the patient to urinary urgency. The three drugs have nearly identical efficacy in prolonging the time to recurrence.99
A randomized trial of intravesical doxorubicin versus BCG in 262 patients with superficial transitional cell carcinoma showed an advantage in the complete response and 5-year disease-free survival rates for those treated with adjuvant BCG.99 A classic series of 86 patients with recurrent superficial bladder cancer prospectively randomized to TURBT plus BCG or TURBT alone was reported by Herr and colleagues.129 Patients treated with BCG had a prolonged median disease-free interval of 24 months compared with 8 months for those patients treated with TURBT alone.129 An update of the data has revealed a 10-year disease-specific survival rate of 75% in the group that received TURBT plus BCG compared with 55% in those treated with TURBT alone. The majority of recurrences were discovered within the first 5 years. Of the 61 patients who received BCG, 33 (54%) were disease free with their bladders preserved.130,131
In a recent review of 11 clinical trials consisting of 2749 patients treated with BCG or mitomycin C, a greater incidence of tumor recurrence was observed for patients treated with mitomycin C compared with BCG (46% versus 36%, respectively). This review also demonstrated improved results with BCG maintenance therapy for reducing the risk of tumor recurrence; however, this is currently controversial because of the potential increased toxicity with BCG maintenance. The incidence of associated cystitis related to intravesical therapy was more prevalent among BCG treated patients (54% versus 39%, respectively).132
The standard of care for superficial bladder cancer with a high risk of recurrence has been established as intravesical BCG. Histologic persistence after 6 months indicates the need to change the intravesicular agent. Disease beyond 1 year indicates the need for a different treatment approach to prevent progression to muscle-invasive cancer. Investigators are testing the application of interferon α.126,133 The role of external-beam radiation in the treatment of CIS is unclear. Especially among patients previously treated with multiple resections and intravesical therapy, the tolerance of external irradiation may be poor because of the pre-existing chronic irritation within the bladder mucosa. Van der Werf-Messing et al.134 have reported excellent control rates (>90%) for limited T1 tumors using interstitial therapy through an open cystotomy approach. In that report, interstitial radium-226 was used with an intended dose of 60 Gy delivered to the visualized bladder tumor. This approach, however, is generally not used in the United States. Patients with persistent CIS or refractory Ta/T1 disease ultimately require cystectomy.
Surgical Treatment of Muscle-Invasive Bladder Cancer
Radical cystectomy in the male implies the en bloc removal of the bladder (with its peritoneal covering), perivesical adipose tissue, lower ureters, prostate gland and seminal vesicles, pelvic vas deferens, proximal urethra, and pelvic lymph nodes (Fig. 44-5). A total urethrectomy is performed for patients with CIS, multicentric tumors, and involvement of the bladder neck or prostatic urethra. A radical cystectomy in female patients is an anterior exenteration with sacrifice of the bladder (with its peritoneal covering), entire urethra, uterus, fallopian tubes, ovaries, anterior vaginal wall, and pelvic lymph nodes. A standard pelvic lymph node dissection generally includes removal of the bilateral external iliac, obturator, internal iliac (hypogastric), and common iliac lymph node chains. The dissection extends from the aortic bifurcation superiorly to the inguinal ligament and node of Cloquet inferiorly and the genitofemoral nerve laterally.135,136 An extended dissection includes all nodes from the standard template plus paracaval, interaortocaval, para-aortic, and presacral lymph nodes. Herr reported on the prognostic effect of nodal status in 637 patients who underwent radical cystectomy and pelvic lymph node dissection.137 For both node-negative and node-positive patients, improved survival and reduced local recurrence related to negative surgical margins and the number of lymph nodes removed at the time of the node dissection. The 5-year survival rates for patients who had 0 to 5, 6 to 10, 11 to 14, and more than 14 lymph nodes removed were 79%, 73%, 44%, and 33%, respectively. The corresponding local relapse rates in these aforementioned nodal groups were 4%, 7%, 8.5%, and 17%, respectively. A multivariate analysis demonstrated that the number of nodes removed was an independent predictor of survival outcome. This observation has been observed in other series and clinical trials.102,103,138 One caveat, however, is that it is not clear if this improved outcome is related to therapeutic removal of occult nodal disease or if it represents a surrogate for the quality of surgery.

Attempts to reduce the morbidity of radical cystectomy have focused on preserving potency in the male and developing urinary diversion alternatives that maximize continence and cosmesis. A nerve-sparing radical cystectomy requires preservation of the neurovascular bundles and the dorsal-venous complex surrounded by the lateral prostatic fascia located posterolateral to the prostatic capsule and membranous urethra.136,139
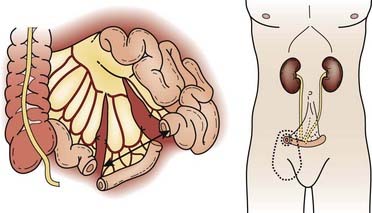
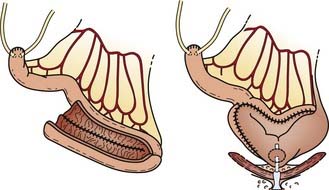
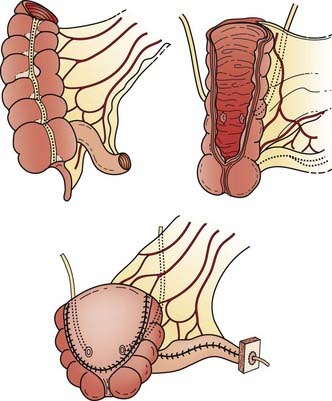
Reconstructive techniques following radical cystectomy generally fall into two categories: incontinent or continent diversions. The standard urinary diversion, an incontinent diversion, is accomplished with a conduit derived from 15 cm of distal ileum to which the ureters are anastomosed (Fig. 44-6). An ostomy is created by attachment of the distal end of the ileum to the defect in the anterior abdominal wall.136 More recently, a second type of urinary diversion, the creation of internal reservoirs, has become available to allow the patient to retain continence. Two classes of continent diversions of the urinary flow are (1) stomal reservoirs that require intermittent catheterization and (2) orthotopic neobladders anastomosed to the remaining distal urethra (Fig. 44-7). There are several techniques for creating a continent cutaneous diversion that can be catheterized including the cecoileostomy (Indiana pouch [Fig. 44-8]) and the ileostomy (Koch pouch). All involve constructing a detubularized pouch from intestine that becomes a spherical reservoir with a constructed sphincter to maintain continence. Because these reservoirs are composed of portions of bowel, metabolic and absorptive disturbances vary depending on the segments and lengths of bowel used.
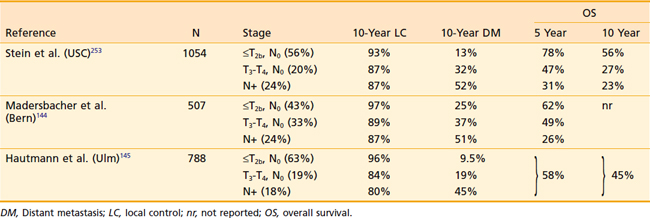
Because of the longer operative times and complexity of these procedures, a higher risk of acute postoperative complications including urinary leak are noted as compared with ileal conduits. By 3 to 4 months the average catheterization interval is decreased to 6 to 8 hours. Nevertheless, the pouch is associated with a 2% mortality, a 5% incidence of serious complications, and a reoperative rate of 30%. Over the past decade, orthotopic neobladder reconstruction techniques have become the preferred method of urinary diversion in appropriately selected patients. Because this reconstruction leaves intact the external urinary sphincter, patients are able to void by performing the Valsalva maneuver. Patients must be carefully chosen for the orthotopic neobladders to avoid incontinence, particularly during sleep, because the guarding reflex is lost with the native bladder. Rates of nocturnal incontinence range from 15% to 40%.140 Five-year survival rates for early stage T2 tumors were often reported to be as low as 17% to 36% before 1980. Patients with stage T3a and T3b tumors had 5-year rates ranging from 18% to 31% and 20% to 25%, respectively. However, more recent studies of cystectomy using modern surgical techniques report survival rates as high as 50% to 88% for T2, 36% to 69% for T3a, and 11% to 47% for T3b tumors.135,141 A summary of recently reported outcomes in large surgical series is summarized in Table 44-2. The overall local control rates with radical cystectomy alone have been reported to be as high as 95%142,143; however, in particular, patients with locally advanced or node-positive disease treated with radical cystectomy alone do not fare as well. Madersbacher et al.144 reported in a recent series of patients treated with radical cystectomy alone isolated local recurrence rates of 9% to 20% for non–organ-confined (T3b-T4) node-negative disease and 13% for node-positive disease. Another surgery-only series reported by Hautmann et al.145 demonstrated local recurrence rates of 16% and 20% in non–organ-confined and node-positive patients, respectively. Of note, this is likely an underestimate of the true local recurrence rates as patients with simultaneous local and distant recurrences are typically included in the metastatic cohort. The overall outcomes of these patients remain suboptimal even in series including neoaduvant and adjuvant therapies. Distant metastases occur in 20% to 50% of patients with locally advanced disease.144,145 For patients with node-positive disease, long-term disease-free survival rates are poor at 25% to 35%.
Preoperative Radiation Therapy
In an effort to improve the outcome for patients with locally advanced bladder cancers treated with surgery, preoperative radiotherapy was commonly used from 1960 to 1980. The rationale for using this approach was to reduce the incidence of tumor bed failures and potential seeding of malignant cells from the operation. Although some retrospective studies have suggested that the addition of preoperative radiotherapy improves the overall outcome,146,147 other series have found no benefit when results are compared with modern surgical series.142,148,149 Several randomized prospective trials that compared preoperative radiotherapy plus radical cystectomy to radical cystectomy alone have demonstrated no significant differences between the treatment arms.150–152 Nevertheless, it must be pointed out that these trials were performed before the improvement in surgical techniques and suffered as well from limited accrual, compromising their power to detect significant differences between the study arms. A review from the M.D. Anderson Hospital supports the notion that preoperative irradiation improves the outcome in a select cohort of patients.153 In this report, 338 patients treated with preoperative radiotherapy between 1960 and 1983 were retrospectively compared with 232 patients treated at the same institution between 1985 and 1990. The majority of the latter group were treated with neoadjuvant or adjuvant chemotherapy. Despite this apparent advantage, there was a significant improvement in local control among patients with T3b disease who received preoperative irradiation. Within this cohort of patients, there was a trend for improved disease-free survival and overall survival, although no significant differences were seen. The use of preoperative radiotherapy in the modern surgical era remains unclear, and at this time is not a standard approach in the United States.
Neoadjuvant/Adjuvant Chemotherapy
Various neoadjuvant regimens have been evaluated in a number of prospective randomized trials. The Nordic Cystectomy I trial evaluated neoadjuvant chemotherapy in combination with low-dose irradiation and cystectomy.154 Patients with T1G3, T2-T4a NXM0 tumors were randomly assigned to either two cycles of chemotherapy with cisplatin and doxorubicin or no chemotherapy before cystectomy. In addition, all patients in this study received radiotherapy (4 Gy/day × 5 days) following the second cycle of chemotherapy. Initial results appeared to show a benefit for neoadjuvant chemotherapy. However, longer follow-up failed to demonstrate a statistically significant difference in overall survival between the two groups (59% versus 51%, P = 0.1).155 Subgroup analysis also demonstrated no survival benefit for patients with T1 and T2 tumors, although patients with T3 and T4a tumors did show a 5-year survival benefit of 52% versus 37% (P = 0.03).
The largest neoadjuvant trial to date was a European study involving more than 900 patients. Between 1989 and 1995, patients with T2G3, T3, and T4a, N0 to NX, M0 tumors were randomized to receive either three cycles of cisplatin, methotrexate, and vinblastine (CMV) neoadjuvant chemotherapy (n = 491) or no chemotherapy (n = 485) before planned cystectomy or definitive radiation therapy (chosen at the discretion of the local treating institution).156 Chemotherapy-associated mortality was 1% and cystectomy operative mortality was 3.7%. Approximately 42% of patients in each arm received radiotherapy as the primary therapy. Although at 4 years no significant difference in overall survival was seen, after longer follow-up (median 7.4 years), a statistically significant 6% absolute survival benefit was found in favor of the chemotherapy-treated patients.157 In addition, the rate of pathologic complete response was found to be dramatically higher in the primary tumors of chemotherapy-treated patients (33% versus 13%).
A similar smaller randomized phase III trial of neoadjuvant methotrexate, vinblastine, doxorubicin (Adriamycin), and cisplatin (MVAC) plus cystectomy (n = 153) versus cystectomy alone (n = 154) was conducted by the U.S. Intergroup in patients with T2 to T4a N0M0 bladder cancer. After a median follow-up of 8.5 years, survival in the MVAC arm was marginally superior, with a hazard ratio of 0.74 (95% CI 0.55-0.99, P = 0.06). The estimated median survival of the MVAC arm was 77 months, while the no-MVAC arm was 46 months.158
Two meta-analyses have been conducted to evaluate the effect of neoadjvuant chemotherapy on overall survival. One meta-analysis of individual patient data consisting of 98% of patients from known randomized trials using cisplatin combination chemotherapy has shown that neoadjuvant therapy provides a moderate but significant benefit in patients with T2-T4a disease. Patients who received neoadjuvant cisplatin combination chemotherapy experienced a 14% reduction in the risk of death (hazard ratio = .86 [CI = .70-.95]) and an absolute improvement in survival of 5% at 5 years.159 Single-agent cisplatin chemotherapy was not shown to provide any survival benefit. A second meta-analysis was conducted that confirmed these results.160 Neoadjuvant cisplatin combination chemotherapy prior to definitive local chemoradiotherapy has been tested in only one study, and did not appear to demonstrate a benefit in favor of chemotherapy. Several other neoadjuvant studies allowed either radiotherapy or cystectomy as local therapy following neoadjuvant chemotherapy. All of these studies have been included in the meta-analyses cited previously, and there was no significant association between the type of local therapy (cystectomy versus radiotherapy) and outcome.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


