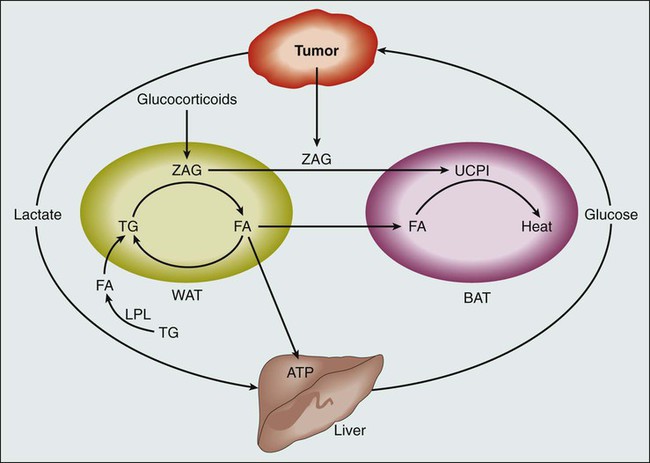
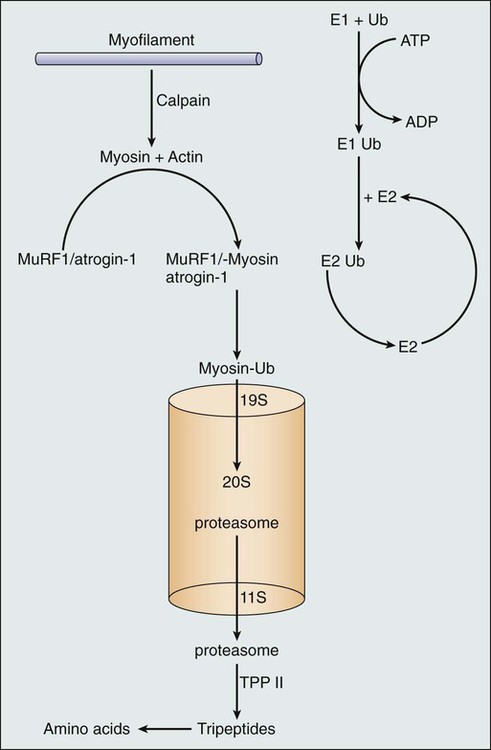
• Loss of appetite and weight loss are common in patients with advanced, incurable cancer and are associated with a poor prognosis. • Although patients with advanced, incurable cancer who have the “cachexia syndrome” may appear malnourished, nutritional support with either enteral or parenteral nutrition rarely provides a positive impact on clinical outcomes. • For palliative purposes, corticosteroids and progestational agents improve appetite in patients with incurable cancer who are experiencing a loss of appetite and weight loss. • A variety of agents that target muscle, including antimyostatin therapy, are currently being tested in clinical trials to begin to determine their role in treating cancer cachexia syndrome. Any list of end-of-life signs and symptoms in patients with cancer includes loss of appetite and loss of weight. This complex of cancer-associated anorexia and weight loss, referred to herein as “cachexia,” is common, arising in more than 80% of patients with cancer who have advanced disease.1 Moreover, it carries ominous ramifications, having a harmful impact on patients’ functional status and leading to increasing debility, and negatively affecting survival itself. Yet despite the high prevalence of cachexia and its detrimental implications, meaningful interventions that improve the appetite, enhance functionality, and improve survival remain lacking in patients with refractory cancer. This chapter specifically focuses on patients with incurable, treatment-refractory metastatic disease. These distinctions of incurability and refractory disease are important. First, previous studies have shown that in the setting of potentially curable cancer, severe malnutrition can be treated with nutrition support and result in improved outcomes.2 However, such is not the case in patients with incurable cancer. Although this latter group of patients may appear “malnourished,” caloric repletion clearly does not lead to improved outcomes and in fact leads to a variety of complications that arise directly from implementing nutrition support. Indeed, as far back as 1989, the American College of Physicians provided a position paper on parenteral nutrition in patients with cancer who are receiving chemotherapy, in which it was stated, “….the routine use of parenteral nutrition for patients undergoing chemotherapy should be strongly discouraged, and, in deciding to use such therapy in individual patients whose malnutrition is judged to be life threatening, physicians should take into account the possible exposure to increased risk.”3 To my knowledge, this position statement has not been revised, emphasizing the ongoing concerns for providing nutrition support to patients with cancer who are at or near the end of life. More recently, Baldwin and colleagues4 conducted a systematic review and metaanalysis that included 13 randomized, controlled studies with 1414 patients with cancer in an effort to assess the role of oral nutritional supplementation. Although enteral nutrition appeared to have some beneficial effect on some aspects of quality of life (e.g., emotional functioning, dyspnea, loss of appetite, and global quality of life), it had no effect on mortality (relative risk = 1.06, 95% confidence interval = 0.92 to 1.22, P = .43; I(2) = 0%; P(heterogeneity) = 0.56). As noted, these studies were fraught with clinical and statistical heterogeneity, and hence these investigators concluded that cachectic patients with cancer or those at risk for cachexia do not appear to gain a survival advantage with oral nutritional support. Once again, the fact that these patients with advanced cancer may appear “malnourished” does not translate into their deriving clear benefit from increased calories. Second, tumor response is often associated with symptom improvement. Geels and colleagues5 showed that among patients with metastatic breast cancer, a higher proportion (91.7%) with a complete or partial response manifested an improvement in anorexia and that none of the patients with a complete response or partial response described a worsening of their appetite.5 Although these results did not reach statistical significance, they point to a phenomenon to which many oncologists can readily attest: tumor response leads to improvements in baseline symptoms in many patients with cancer. Hence this chapter focuses on a commonly seen group of patients with cancer who are cachectic and who experience symptoms and signs that are refractory to cancer treatment and caloric repletion. From an epidemiological standpoint, is cachexia truly a concern for patients, their families, and health care providers? A classic article from the Eastern Cooperative Oncology Group demonstrates that it is a concern. Dewys and colleagues6 used prospectively gathered data from 12 cancer cooperative group trials that in total included more than 3000 patients with cancer and showed that patients who lost weight lived shorter lives. A patient-reported weight loss of >5% over the preceding months was a powerful predictor of early demise. In multivariate analyses that included cancer type, tumor burden, and patient performance status, patients with weight loss that exceeded this 5% threshold died sooner than did patients who indicated that they had been able to maintain their weight. This study has been replicated by other investigators and demonstrates the strong negative prognostic effect of cachexia. This same prognostic effect is seen with patient-reported decline in appetite. Quinten and colleagues7 examined 30 randomized controlled trials from the European Organisation for Research and Treatment of Cancer from 1986 through 2004 including more than 1800 patients with cancer who described varying degrees of appetite loss.7 Median survival was directly tied to better appetite; patients with no appetite loss had a much more favorable median survival compared with patients who lost some degree of their appetite. Moreover, these investigators described a fairly direct relationship between extent of appetite loss and shorter survival. Hence not only is weight loss a strong predictor of poor outcome in patients with metastatic cancer, but the same can be said for appetite. To date, most research has underscored the fact that cancer itself is the main culprit when it comes to losing weight in the setting of advanced malignancy. Several studies point to the predisposition of patients with cancer to lose lean tissue with some slight preservation of adipose tissue, a clinical scenario that stands in stark contrast to what one observes in classic cases of starvation, in which adipose tissue wastes and lean tissue is relatively preserved. Recently, however, findings of a series of studies suggest that some of the newer cancer agents lead to the direct wasting of lean tissue, despite their role in sometimes improving patient survival. For example, Antoun and colleagues8 recently undertook a secondary analysis of data from a placebo-controlled, double-blind trial in patients with metastatic renal cell carcinoma who were treated with sorafenib, 400 mg twice a day. The findings of these investigators, who used retrospective analyses of computed tomographic images, were surprising. As expected, at study entry, muscle wasting was observed in 72% of patients who presented with a body mass index of less than 25 and in 34% of patients with a body mass index greater than 25. However, although patients in the placebo group presented with stable body weight during 6 months with no major changes in body composition, patients who received sorafenib lost on average 2.1 kg of weight over 6 months and 4.2 kg over 1 year. Moreover, patients treated with sorafenib lost skeletal muscle progressively at 6 months (a decrease of 4.9%; P = .01) and 12 months (a decrease of 8.0%; P = .01), and statistically significant decrements in muscle mass were observed even in comparisons against the placebo arm. An emerging literature suggests that some of the newer targeted cancer agents have unexpected and possibly detrimental effects on the body composition of patients with cancer. Further research in this area is indicated. Understanding the biological pathways that lead to cachexia has been difficult (Fig. 41-1). From a pathophysiological standpoint, we know that the clinical picture associated with cachexia represents a disease state as opposed to a potentially readily reversible entity, such as that seen with starvation. Three observations substantiate this statement. First, as alluded to earlier, the changes in body composition in a cancer-laden state are different from those seen during starvation. Cohn and colleagues9 used a variety of body composition assessment techniques, including prompt gamma neutron activation, total body potassium measurement, and total body water assessment by means of tritiated water. Such technology, when applied to patients both with and without cancer, resulted in the following observations: (1) patients with cancer lose both muscle mass and fat mass; (2) patients with cancer appear to retain fat mass to a notable degree; and (3) skeletal muscle is lost appreciably. As noted earlier, the opposite scenario occurs in the setting of classic starvation, in which individuals lose fat and retain lean tissue. Second, for reasons that remain unexplained, some groups of patients with cancer manifest an increase in resting energy expenditure. Results have at times been inconsistent, but several studies indicate that patients with cancer engage in an unintentional, futile utilization of energy stores when they are at rest. In otherwise healthy individuals, in the setting of starvation, these observations do not hold true, and in fact, such individuals manifest a drop in resting energy expenditure, presumably in an effort to retain energy stores. Third, in contrast to simple starvation, cachexia from cancer is associated with a loss of appetite. Patients with cancer who are in the throes of this syndrome generally do not crave food and in fact sometimes have developed an aversion to it. Again, observations such as the three previously outlined draw a sharp distinction between cancer cachexia and simple starvation. What processes, at a cellular level, explain these observations? Although much work remains to be done to elucidate these processes, a series of laboratory-based studies have suggested that cachexia is driven by inflammatory cytokines, which in turn activate the ubiquitin proteasome system with subsequent muscle breakdown10 (Fig. 41-2). However, small-scale, clinically based interventional studies that have used either cytokine blockade or proteasome inhibition have not demonstrated favorable clinical outcomes.11,12 Other laboratory-based investigators have suggested different mechanisms to explain cancer-associated wasting of lean tissue. For example, a high-profile study described a proteolysis inhibiting factor, but subsequent, more clinically based studies have raised questions regarding the clinical relevance of proteolysis inhibiting factor.13,14 In essence, the pathophysiology of cachexia continues to be studied at a cellular level, but clinical validation of these findings remains elusive.
Cancer Cachexia
Introduction
Definitions and Epidemiology
Biological Characteristics and Pathophysiology
Oncohema Key
Fastest Oncology & Hematology Insight Engine