Developing a successful cancer center within the community is achievable. This article provides an understanding of the standards and guidelines of the Commission on Cancer (CoC), the different community cancer center program categories, and the accreditation process. The pivotal roles of institutional support and physician leadership in the development of a successful cancer center have been elucidated.
The development of a successful cancer center program is not limited to an academic environment; in fact, more than 85% of patients in the United States will receive their initial diagnosis or care at a community cancer center. The creation and improvement of community cancer programs is critical to the advancement of cancer care in this country. Among their many functions, cancer centers promote excellence in cancer care in the community, apply national normative standards of care, optimize the delivery of care, improve access to clinical trials, and measure and report cancer metrics to entities such as the National Cancer Database.
Historically, formal processes for continuously understanding, managing, and controlling cancer have been driven by surgeons through the mechanisms of the American College of Surgeon’s (ACS) Commission on Cancer (CoC). Established in 1922, the ACS CoC was formed as a consortium of professional organizations dedicated to improving survival and quality of life for patients with cancer through standard-setting, prevention, research, education, and monitoring of comprehensive quality of care.
Standards for the evaluation of cancer clinics and registries were first published in 1930 by the ACS Committee on the Treatment of Malignant Disease. The first surveys of cancer clinics were conducted in 1931. Continuously revised and expanded, these standards define the development process for a cancer program. The most recent standards were published in 2009.
This introductory article provides a primer for understanding the mechanism for building a community-based cancer program. The pillars of this process include understanding established standards and guidelines of the CoC, the different community cancer program categories, the accreditation process, the role of physician leadership, and the need for institutional support. The seven CoC cancer programs applicable to the community setting and the requirements for accreditation in each are explored. For a more thorough and complete description, the reader is directed to the ACS CoC guidelines.
Cancer center versus cancer program
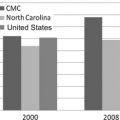
Large academic cancer centers have no monopoly on the treatment of cancer. For instance, although the NCI Cancer Center Programs make significant contributions in cancer research that are key to understanding, preventing, and treating this disease, only 15% of patients in the United States are diagnosed and receive their initial treatment at NCI-designated cancer centers. Thus, 85% of cancer care is provided in the community setting. According to CoC statistics for 2010, 71% of cancer care is provided in one of the 1400 CoC accredited programs.
The term cancer center is neither codified nor copyrighted. According to Simone, a cancer center is best described as “a formal organization of diverse and complimentary specialists who work on the cancer problem together and simultaneously rather than serially. The center is under sufficient central authority to focus efforts and organize resources for the efficient and synergistic accomplishments of its goals in patient care and/or research.” This term suggests a physical proximity of services that complements the efficient and reproducible delivery of care.
A cancer program extends the cancer center concept dramatically. A cancer program not only addresses the significant and immediate needs of diagnosis and treatment but also provides community screening, long-term follow-up with data registry reporting, and posttreatment surveillance. In addition to meeting the needs of the patient, a cancer program provides cancer education to the community and disease-specific certification to the medical staff.
The accreditations program
Through the CoC Accreditations Program, any hospital or treatment center that seeks to improve the quality of care within its community can voluntarily commit to comply with CoC standards designed for facilities of similar size. After conforming to the guidelines (discussed later) a program can then apply for accreditation. Accreditation is granted only to facilities that have undergone a thorough and rigorous evaluation and performance review for compliance with the CoC standards. To maintain accreditation, facilities with accredited cancer programs must undergo an on-site review every 3 years.
All hospitals and freestanding treatment facilities are eligible to participate in the CoC Accreditation Program. The five elements key to the success of a CoC Accredited Cancer Program are (1) clinical services, (2) cancer committee/leadership body, (3) cancer conferences, (4) quality improvement program, and (5) cancer registry and database. By design, compliance with the CoC standards established for any one of the CoC-defined cancer program categories ( Table 1 ) promotes improved patient care.
| Program | Required Category Goals | Required Coordinators | Minimum Number of Newly Diagnosed Cancer Cases | Minimum Required Percentage Accrual to Clinical Trials |
|---|---|---|---|---|
| Network Cancer Program (NCP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | None | 8% |
| NCI-designated Comprehensive Cancer Program (NCIP) | Cancer conference Clinical Quality improvement | None | None | Exempt |
| Teaching Hospital Cancer Program (THCP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | None | 4% |
| Veterans Affairs Cancer Program (VACP) | Clinical Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement, For facilities that qualify, ad hoc or Veterans Integrated Service Networks–assigned coordinators are appointed | None | 2% |
| Pediatric Cancer Program (PCP) | Clinical Clinical research Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Child life or long-term follow-up | None | 4% |
| Pediatric Component Cancer Program (PCPC) | Clinical Clinical research Programmatic endeavors Quality improvement | Facility coordinators responsible for activities of the pediatric cancer program Pediatric cancer conference Child life or long-term follow-up | 50 | 4% |
| Community Hospital Comprehensive Cancer Program (COMP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference, quality of cancer registry data, quality improvement, community outreach | 650 | 2% |
| Community Hospital Cancer Program (CHCP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | 100–649 | Exempt |
| Hospital Associate Cancer Program (HACP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | 50–99 | Exempt |
| Affiliate Hospital Cancer Program (AFCP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | Less than 50 | Exempt |
| Integrated Cancer Program (ICP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | None | Exempt |
| Freestanding Cancer Center Program (FCCP) | Clinical Community outreach Programmatic endeavors Quality improvement | Cancer conference Quality of cancer registry data Quality improvement Community outreach | None | Exempt |
Related posts:
 Breast Conservation Therapy Versus Mastectomy in the Community-Based Setting: Can This Rate Be Used as a Benchmark for Cancer Care?
Breast Conservation Therapy Versus Mastectomy in the Community-Based Setting: Can This Rate Be Used as a Benchmark for Cancer Care?
 American College of Surgeons Oncology Group and the Community Surgeon
A Community Hospital Clinical Trials Program: Infrastructure for Growth
American College of Surgeons Oncology Group and the Community Surgeon
A Community Hospital Clinical Trials Program: Infrastructure for Growth
 Maximizing Rectal Cancer Results: TEM and TATA Techniques to Expand Sphincter Preservation
Minimally Invasive Esophagectomy in the Community Hospital Setting
The National Accreditation Program for Breast Centers: Quality Improvement Through Standard Setting
Maximizing Rectal Cancer Results: TEM and TATA Techniques to Expand Sphincter Preservation
Minimally Invasive Esophagectomy in the Community Hospital Setting
The National Accreditation Program for Breast Centers: Quality Improvement Through Standard Setting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


