Figure 130.1 Algorithm for the evaluation and treatment of subacute brucellosis.
In this form of the disease, the 2-mercaptoethanol test detects IgG, and titer above 1:80 defines active infection. Brucella are isolated in 40% to 70% of serial blood cultures; the bone marrow culture (0.5 to 1 mL of aspirate from the iliac crest) permits isolation in 90% of these patients.
Chronic brucellosis (Figure 130.2)
In the chronic form with more than 1 year of illness, there usually is an afebrile pattern with myalgia, fatigue, depression, arthralgias, and so on. The most important differential diagnosis is chronic fatigue syndrome.
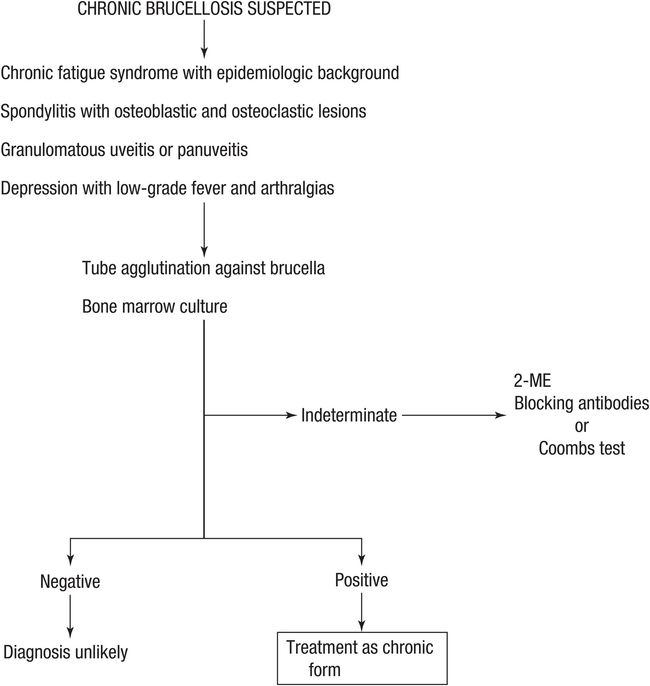
Figure 130.2 Algorithm for the evaluation and treatment of chronic brucellosis. 2-ME = 2-mercaptoethanol.
Other localized forms are granulomatous or recurrent uveitis and spondylitis. Peripheral arthritis and sacroiliitis are rare.
This form of disease is produced mainly by B. melitensis. It is found mainly in adults older than 30 years of age, especially older than 50 years old, and is rare in children.
The routine serologic tests and blood cultures give a diagnosis only 10% to 20% of the time. We recommend Coombs test specific for Brucella or blocking antibodies. The bone marrow in our experience produces a positive culture in 50% to 75% of patients.
Therapy
The intracellular character of Brucella results in an important therapeutic challenge, especially in subacute and chronic forms. Antibiotics should have in vitro activity, but the intracellular concentration must be adequate.
Tetracyclines have shown excellent in vitro activity throughout the world. The MIC90 (minimum inhibitory concentration required to inhibit growth of 90% of the organisms) was 2 μg/mL for tetracycline and 0.125 μg/mL for doxycycline in our surveillance in Peru. During the past 25 years, the antibiotic activity pattern of tetracycline against B. melitensis has not changed, which is remarkable because these are still our drugs of choice.
In addition, for oxytetracycline and doxycycline the minimal bactericidal concentration (MBC) was equal to MIC. All these features in conjunction with worldwide experience point to tetracyclines as the keystone of treatment.
The differences among tetracyclines are tolerance, dosage, and safety profile; however, the new ones have better tolerance and fewer side effects and can be used with meals without reducing efficacy. We prefer to use doxycycline or minocycline.
The other important aspect is the need to combine antibiotics to reduce the rate of relapse. Most antibiotics can reduce the fever, but recurrence is high.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


