Breast Lesions in Children and Adolescents
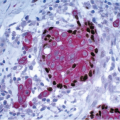
The prepubertal breast in both boys and girls consists primarily of lactiferous ducts that exhibit some branching without evidence of progressive alveolar differentiation, although some rudimentary lobular structures may be seen. The breast is maintained in this state until the time of puberty. Extramedullary hematopoiesis in the stroma, a feature seen in the fetal breast, may persist until 4 months of age (Fig. 17.1, e-Fig. 17.1).1
At puberty in females, there is duct elongation, branching, and development of a thickened epithelium, which is primarily due to the influence of estrogen.2 This is accompanied by an increase in the density of periductal connective tissue, which is also the result of relative estrogen dominance. Deposition of stromal adipose tissue also occurs, and it is this adipose tissue that is largely responsible for the enlargement and protrusion of the breast disc at this time. Cyclical exposure to progesterone following exposure to estrogen during ovulatory cycles promotes lobulo-acinar growth as well as connective tissue growth. Although the majority of lobulo-acinar development occurs during puberty, this process continues into the third decade and terminal differentiation of the breast is induced only by pregnancy.
The adolescent male breast is composed of fibroadipose tissue and ducts lined by low cuboidal epithelial cells.
A number of breast lesions that occur in adults may be seen in children and adolescents, including fibroadenomas, phyllodes tumors, and intraductal papillomas. Gynecomastia may be seen in adolescent boys, as discussed in Chapter 16. This chapter will focus on several lesions that are primarily seen in children and adolescents.
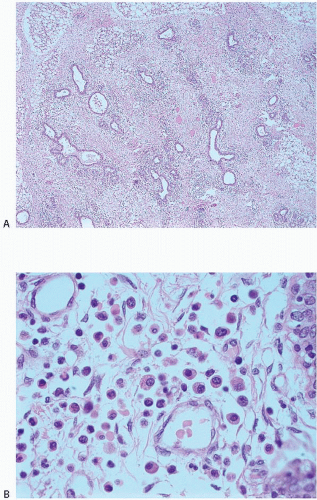 FIGURE 17.1 A: Low-power view of breast tissue from a neonate showing ducts embedded in a stroma composed of loose connective tissue and adipose tissue. The stromal mononuclear cells are hematopoietic elements, which is indicative of persistent extra medullary hematopoiesis. B: High-power view demonstrating hematopoietic cells in the stroma (courtesy of Dr. Theonia K. Boyd). |
JUVENILE (VIRGINAL) HYPERTROPHY
Rapid and distressing enlargement of one or frequently both breasts may occasionally occur in adolescence. Careful clinical history and physical examination are required, particularly in patients with unilateral enlargement, to prevent the interpretation of this lesion as a tumor which, in turn, could result in inadvertent surgical removal of the developing breast disc. Histologic examination shows features similar to those of gynecomastia, with abundant connective tissue and duct proliferation, frequently with epithelial hyperplasia, but with little or no lobule formation.3
Reduction mammaplasty is usually the treatment of choice. Recurrences have been reported and may require a second mammaplasty procedure or even mastectomy with reconstruction. Recurrences are more common if hypertrophy developed early in puberty.4
JUVENILE FIBROADENOMA
Most fibroadenomas that occur in the adolescent female are histologically similar to those presenting in older women. The term juvenile fibroadenoma refers to a distinct lesion characterized by a rapid growth phase that more commonly occurs in postpubertal children and usually attains a larger size than the fibroadenomas seen in adults. The histologic features of this entity are discussed in Chapter 6.
JUVENILE PAPILLOMATOSIS
Juvenile papillomatosis, as the name implies, is a disorder that usually occurs in young women, most often in those <30 years of age. Two-thirds of the reported patients have been <25 years of age. However, the lesion has been noted in patients as young as 12 and as old as 48 years.5
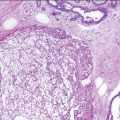
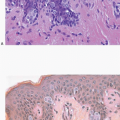
This lesion presents as a well-defined, firm mass often mistaken clinically for a fibroadenoma. Gross examination shows cysts of varying size, which impart a Swiss cheese-like appearance to the specimen on cut section. Microscopically, juvenile papillomatosis is characterized by a combination of cysts and ectatic ducts, which may contain inspissated secretions and intraluminal foamy histiocytes, epithelial hyperplasia and papillomatosis, and apocrine metaplasia. Fibroadenomatous change and sclerosing adenosis may also be seen (Figs. 17.2, 17.3, 17.4 and 17.5, e-Figs. 17.2, 17.3 and 17.4




Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
