Malignant bowel obstruction (MBO) was defined using the following criteria: clinical evidence of bowel obstruction (history/physical/radiologic examination); bowel obstruction beyond the ligament of Treitz, in the setting of a diagnosis of intra-abdominal cancer with incurable disease; or a diagnosis of non-intra-abdominal primary cancer with clear intraperitoneal disease (1,2).
MBO is a common complication in patients with abdominal or pelvic cancers, such as those arising from colon, ovary, and stomach. Bowel obstruction occurs in patients with a diagnosis of advanced primary or metastatic intra-abdominal malignancy such as ovarian cancer (5.5% to 51%) and colorectal cancer (10% to 28%) (3,4). MBO has also been reported in patients with non-intra-abdominal cancers, such as melanoma, breast cancer, and lung cancer (5). The interval from diagnosis of cancer to onset of MBO is significantly longer between intra-abdominal (mean 22.4 months) and extraabdominal primary tumors (mean 57.5 months) (5,6,7,8,9,10).
Pancreatic cancer spreads directly to the duodenum or stomach; cancer of the colon spreads to the jejunum and ileum; and prostate and bladder cancers spread to the rectum (11). Tumors at the splenic flexure can cause bowel obstruction in 49% of cases, tumors of right and left colon in 25% of cases, and tumors of the rectum and rectosigmoid junction in 6% of cases (11).
Bowel obstruction may be partial or complete, and at single or multiple sites, the small bowel is more commonly involved than the large bowel (61% vs. 33%) and both are involved in over 20% of the patients. Even in advanced cancer, the obstruction may be due to benign causes such as adhesions, postirradiation bowel damage, inflammatory bowel disease, hernia, or intussusceptions of the bowel. Some reports suggest that a benign cause is responsible for obstruction in about 48% of the patients with colorectal cancer (2,3,11,12,13).
Cancer patients may develop bowel obstruction at any time in their clinical history: at the time of diagnosis of the malignancy or as part of recurrent disease, sometimes associated with an end-of-life state.
PATHOPHYSIOLOGY
Several physiopathologic mechanisms and causes may be involved in the onset of bowel obstruction and there is variability in both presentation and etiology.
Mechanical obstruction is caused by the following: (1) extrinsic occlusion of the lumen due to an enlargement of the primary tumor or recurrence, mesenteric and omental masses, and abdominal or pelvic adhesions (caused by either the tumor or secondary to surgery), postirradiation fibrosis; and postirradiation intestinal damage; (2) intraluminal occlusion of the lumen due to neoplastic mass, polypoidal lesions, or annular tumoral dissemination; (3) intramural occlusion of the lumen due to intestinal linitis plastica.
Functional obstruction (or adynamic ileus) is caused by intestinal motility disorders consequently to: (1) tumor infiltration of the mesentery or bowel muscle and nerves (peritoneal carcinomatosis), malignant involvement of the celiac plexus; (2) paraneoplastic neuropathy in patients with lung cancer; (3) chronic intestinal pseudo-obstruction mainly due to diabetes mellitus, previous gastric surgery, and other neurologic disorders; and (4) paraneoplastic pseudo-obstruction.
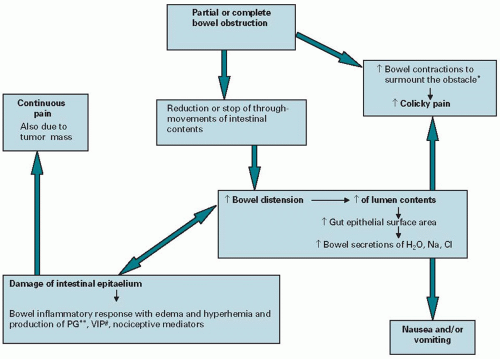
At least four factors occur in bowel obstruction: (1) accumulation of gastric, pancreatic, and biliary secretions that are a potent stimulus for further intestinal secretions; (2) decreased absorption of water and sodium from the intestinal lumen; (3) increased secretion of water and sodium into the lumen as distension increases; and (4) bowel wall edema proximal to the level of the obstruction secondary to inflammation (Figure 15.1). These factors produce a vicious circle of secretion-distension-secretion-motor hyperactivity. Depletion of water and salt in the lumen is considered the most important “toxic factor” in bowel obstruction (11,13).
Clinical and Radiologic Diagnosis
In cancer patients, compression of the bowel lumen develops slowly and often remains partial. Symptoms become more frequent and last longer until near to complete obstruction results. Initial management includes a clinical assessment to rule out acute causes of obstruction and to ensure that the patient does not have a surgical emergency. Gastrointestinal (GI) symptoms such as pain at the tumor site, abdominal cramps, nausea and vomiting, abdominal distension are caused by the sequence of distension-secretion-motor activity of the obstructed bowel. The symptoms occur in different combinations and intensity depending on the site of obstruction (Figure 15.1) (Table 15.1) (9,10,11,13,14). In order to be able to diagnose the condition in a proper manner, a complete clinical history and a physical examination are mandatory before any investigation is ordered.
Figure 15.1. Pathophysiology of bowel obstruction.
The symptoms referred to by the patient should be monitored daily. Vomiting can be evaluated in terms of quantity, quality, and number of daily episodes. Other symptoms such as nausea, pain, dry mouth, drowsiness, dyspnea, hunger, and thirst can be assessed by numerical or verbal scales.
Radiologic imaging in the evaluation of patients with the acute abdomen and the confirmation of the diagnosis of MBO have assumed a pivotal role. The preferred radiologic procedure has evolved in recent years, but it varies in different parts of the world according to the local expertise and the availability of each imaging modality.
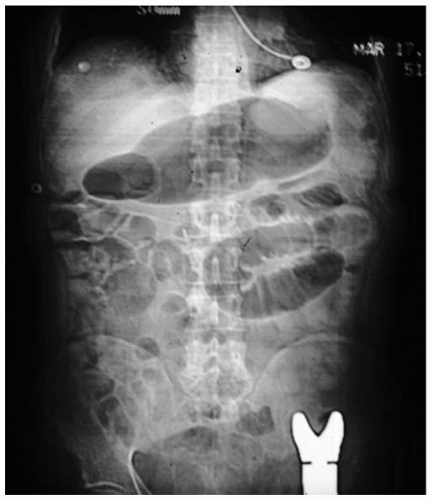
For decades, plain abdominal radiography taken in the supine and standing positions has been the standard in the initial evaluation of patients with acute abdominal pain or suspected obstruction, but its usefulness in the present era is questionable (Figure 15.2). Plain radiography can document the air-filled dilated loops of bowel, differential airfluid levels, or both, but the accuracy for localizing the point and cause of obstruction is low. The sensitivity of plain films in making a diagnosis of small bowel obstruction has been reported to be as low as 66% (15). Despite this, it remains an important step in the evaluation of most patients with acute and chronic abdominal symptoms.
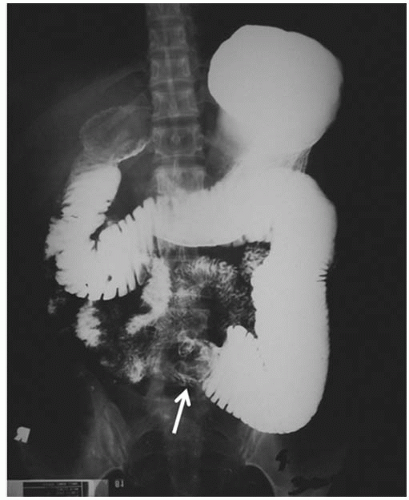
Contrast GI series using barium suspensions provide excellent radiologic definition of the mucosal pattern and luminal patency, particularly in the assessment of the stomach and proximal small bowel (Figure 15.3), but more distal points of small bowel obstruction may not be seen as clearly due to the difficulty in the barium reaching this far in the small bowel and the effects of retained luminal fluid. As it is not absorbed, the retention of barium in the lumen, and the inability to subsequently eliminate it in the setting of obstruction, can then interfere with subsequent radiographic studies. For these reasons, barium small bowel series should be used selectively, and preferably, for evaluating more chronic symptoms or for searching the cause of persistent intestinal symptoms when acute obstruction has already been ruled out.
In the evaluation of large bowel obstruction, barium enema provides a quick, accurate, and inexpensive assessment of the location and cause of obstruction. This, however, should be performed with caution to avoid excessive insertion of barium proximal to the point of obstruction, as this can lead to retention of the barium proximal to the obstruction leading to dehydration of the barium and potential impaction. This is especially a problem in patients with incomplete and inoperable large bowel obstruction. Similarly, if large bowel obstruction is suspected on initial plain abdominal X-rays, a small bowel series should not be performed to avoid the barium from becoming trapped in the proximal obstructed regions of the colon.
TABLE 15.1 Common symptoms in cancer patients with malignant bowel obstruction
Vomiting
Intermittent or continuous
It develops early and in great amounts in gastric, duodenum, and small bowel obstruction and develops later in large bowel obstruction
Biliary vomiting is almost odorless and indicates an obstruction in the upper part of the abdomen. The presence of bad smelling and fecaloid vomiting can be the firstsign of an ileal or colic obstruction
Nausea
Intermittent or continuous
Colicky pain
Variable intensity and localization due to distension proximal to the obstruction; secondary to gas and fluid accumulation most of which are produced by the gut
If it is intense, periumbilical, and occurring at brief intervals may be an indication of an obstruction at the jejunum-ileal level. In large bowel obstruction, the pain is less intense, deeper, occurring at longer intervals, and spreads toward the colon wall
An overall acute pain that begins intensely and becomes stronger or a pain that is specifically localized, may be a symptom of a perforation or an ileal or colic strangulation. A pain that increases with palpation may be due to peritoneal irritation or the beginning of a perforation
Continuous pain
Variable intensity and localization
It is due to abdominal distension, tumor mass, and/or hepatomegaly
Dry mouth
It is due to severe dehydration, metabolic alterations, and above all it is due to the use of drugs with anticholinergic properties and poor mouth care
Constipation
Intermittent or complete
In case of complete obstruction, there is no evacuation of feces and no flatus
In case of partial obstruction, the symptom is intermittent
Overflow diarrhea
It is the result of bacterial liquefaction of the fecal material
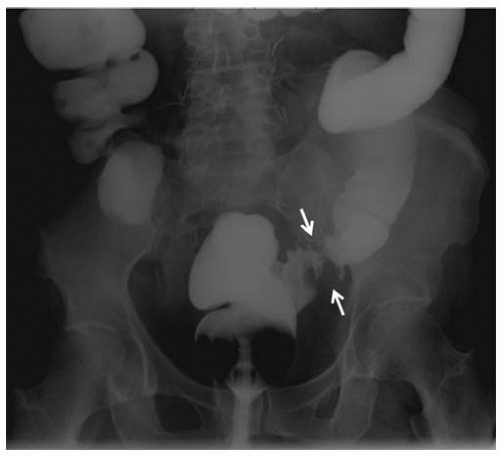
Gastrografin (diatrizoate meglumine) may also be useful in evaluating small and large bowel obstructions (Figure 15.4), but it usually only provides good visualization of proximal small bowel obstruction as the water soluble nature of the Gastrografin will result in it being diluted by the excess fluid retained in the distal small bowel.
Enteroclysis (the small bowel enema) requires the insertion of a long nasoenteric tube, which is manipulated under fluoroscopy guidance beyond the stomach by the radiologist. The contrast is then inserted under pressure resulting in full distension of the loops of small bowel, permitting better assessment of the mucosal pattern and patency, and improving the accuracy of diagnosis in small bowel obstruction. The discomfort associated with the procedure results in the need for it to be done with the use of sedatives. Unfortunately, as it requires radiologists with expertise in the technique, it is not widely available. Transcutaneous ultrasonography has been used successfully in making the diagnosis of MBO, but it has limited usefulness when bowel loops are filled with air. It is also more operator dependent and is therefore less utilized for this indication in the United States than in Europe.
Although the diagnosis and location of obstruction can, at times, be suggested by the history, physical examination, and plain or contrast radiography, oncology patients often have altered GI motility caused by the use of narcotics and antidiarrheal agents or certain chemotherapeutic agents that can result in a paralytic ileus. This may confuse the initial presentation, resulting in a delay of diagnosis and initiation of treatment. Cross-sectional imaging by computed tomography (CT) scanning (Figure 15.5) or magnetic resonance imaging (MRI) has now been shown to provide superior results in the assessment of abdominal symptoms and in the diagnosis of bowel obstruction. Maglinte et al. (16) advise the initial use of abdominal CT scanning for the evaluation of patients presenting with acute abdominal symptoms that are suggestive of obstruction, but use of enteroclysis or small bowel fluoroscopic GI follow-through examinations for the evaluation of mildly symptomatic patients or those with chronic or intermittent complaints.
Figure 15.2. Plain abdominal X-ray image of a patient with obstructing metastasis from renal cancer. Dilated small bowel loop seen, but cause or severity not clearly determined. (Image kindly provided by Dr. Mark Gollub, MSKCC.)
Figure 15.3. Barium gastrointestinal series image demonstrating high-grade, malignant-appearing, small bowel obstruction from a primary jejunal cancer (arrow). (Image kindly provided by Dr. Mark Gollub, MSKCC.)
Figure 15.4. Gastrografin enema image of a patient with ovarian cancer causing partial sigmoid colon obstruction, shown between the arrows.
Comparative studies have demonstrated superior results with cross-sectional imaging in accurately predicting the cause of symptoms. The diagnostic accuracy for determining the cause of obstruction was reported to be 87% for CT, 23% for ultrasound, and 7% for plain film radiography (17). Newer technology in CT scanning such as spiral and multidetector scanners provides a better global assessment of the abdomen and pelvis and when coupled with multiplanar reconstruction can help focus on the transition point in bowel obstruction, thereby helping determine the site, cause, and severity of obstruction (Figure 15.6) (18). CT scanning also provides a greater appreciation for the integrity of the bowel wall proximal to the obstruction, helping to predict the existence of ischemia, pneumatosis, or early perforation with greater accuracy than other modalities.
A recent report by Angelilli et al. (19) demonstrated a sensitivity, specificity, and accuracy for CT scan of 74%, 100%, and 92%, respectively, in confirming a neoplastic cause of MBO. Multidetector computed tomography scanning has also been shown to be highly accurate in identifying the malignant cause of colonic obstruction and in identifying specific features such as the presence of air-fluid levels in the colonic lumen, mural pneumatosis, and a right colon diameter of >10 cm as poor prognostic features (Figure 15.7) (20). These features help expedite making a decision on management, which can sometimes be critical in the overall prognosis for patients with strangulating bowel obstruction.
MRI may also provide similar diagnostic information, but it is not as widely available as CT scanning and local expertise in its use in the assessment of bowel obstruction is limited. The strength of MRI is the absence of radiation exposure, so in the pediatric population, especially in those with chronic or recurrent GI symptoms, such as in patients with inflammatory bowel disease, it is becoming the preferred modality of repeated imaging. The expected results with MRI should be similar to CT scanning, but the data on the sensitivity, specificity, and accuracy are still awaited.
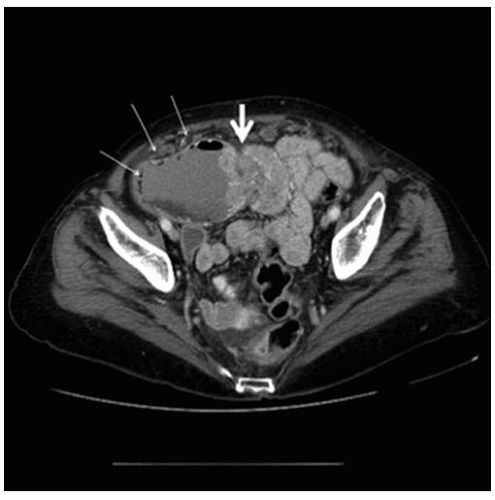
Figure 15.5. A: Computed tomography scan image of a patient with malignant bowel obstruction caused by metastasis from renal cancer (same patient as in Figure 15.2) showing the dilated jejunal loop. B: Subsequent image showing obstructing mass causing intussusceptions (arrow). (Images kindly provided by Dr. Marc Gollub, MSKCC.)
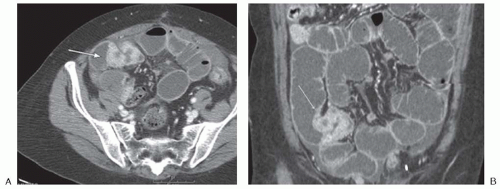
Figure 15.6. A and B: Axial and coronal reconstruction images of a computed tomography scan in a patient with malignant small bowel obstruction from an ovarian cancer implant (arrow). (Images kindly provided by Dr. Mark Gollub, MSKCC.)
Figure 15.7. Computed tomography scan image of an obstructing small bowel metastasis (large arrow) with edema and pneumatosis (small arrows) of the jejunal wall. (Image kindly provided by Dr. Mark Gollub, MSKCC.)
THERAPIES
The management of patients with MBO is one of the greatest challenges for physicians who care for cancer patients. The approach to management of the patient with MBO is completely different in each situation. Although MBO is usually associated with advanced-stage disease when it occurs at the time of initial diagnosis, regardless of the primary site of malignancy, management generally proceeds with curative intent and each patient should be managed according to appropriate principles/guidelines for the underlying malignancy. On the other hand, MBO as part of recurrent disease is often managed with palliative intent; in this context, different factors should be considered to determine the most appropriate treatment.
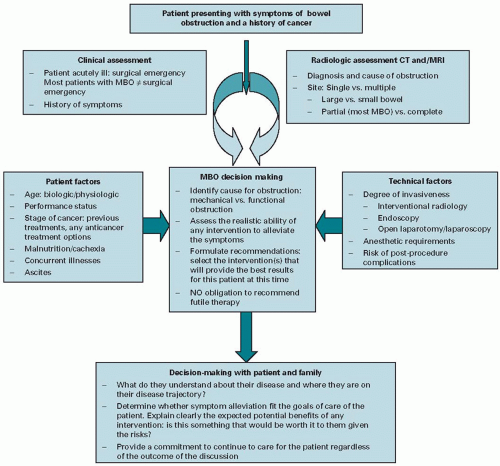
Figure 15.8. Algorithm for assessing and managing a patient with malignant bowel obstruction. MBO, malignant bowel obstruction; CT, computed tomography; MRI, magnetic resonance imaging.
For patients with recurrent disease, MBO generally occurs in a chronic and slow fashion that results in narrowing of the diameter of the small or large bowel (or both simultaneously).
In the face of a clearly incurable situation, significant patient discomfort and suffering must be balanced with the need to simplify the care of those patients with a short time to live. The goal in any decision we make needs to impact the quality of life (QOL) of the affected person in a positive way and each assessment and management needs to be tailored to the specific needs of the patients. Figure 15.8 shows the algorithm for assessing and managing a patient with MBO. The physicians need to consider a series of questions when faced with terminal cancer patients (patients are no longer responsive to specific oncologic therapies) with bowel obstruction: Is the patient fit for surgery? Is there a place for stenting? Is it necessary to use a venting nasogastric tube (NGT) in inoperable patients? When should a venting gastrostomy be considered? What drugs are indicated for symptom control? What is the proper route for drug administration? What is the role of parenteral hydration and total parenteral nutrition (PN)? Figure 15.8 shows the algorithm for assessing and managing a patient with MBO.
Endoscopic Management of Gastroduodenal and Proximal Jejunal Obstruction
Gastric outlet obstruction (GOO) and small bowel obstruction are very debilitating presentations of malignancy that are commonly seen in patients with pancreatic cancer, distal gastric cancer, gall bladder cancer, and cholangiocarcinoma. This can also result from metastases of a variety of extraabdominal malignancies, such as breast cancer and lung cancer. Although GOO is technically not considered MBO, it will be discussed here as it is a common source of morbidity in cancer patients and is managed in a manner similar to other forms of MBO. Advances in endoscopic techniques have now permitted the treatment of this problem to be readily accomplished with the endoscopic insertion of a self-expanding metal stent (SEMS) (Figure 15.9) or gastric venting via a percutaneously placed gastrostomy (drainage percutaneous endoscopic gastrostomy [PEG]). These approaches are particularly useful for patients with limited expected survival.
Figure 15.9. Radiographic and endoscopic images of a patient with malignant duodenal obstruction treated with endoscopic stenting. A: Computed tomography scan demonstrating dilated stomach and transition point in duodenum. B: Endoscopy showing obstructed pylorus. C: Endoscopy image after insertion of stent. D: Barium gastrointestinal series after stent insertion demonstrating relief of obstruction.
The procedure is easily performed using techniques similar to those used for inserting bile duct stents in patients with obstructive jaundice, but it has still not become widely available except at university or cancer centers with interventional endoscopists. The technical success rates for placement of enteral stents have been reported to be >90% and clinical success for resolution of nausea and vomiting with improved ability to consume food orally is reported over 75% (21,22,23,24,25) (Table 15.2).
TABLE 15.2 Summary results from two multicenter studies of endoscopic stent placement for treatment of malignant gastroduodenal obstruction
In the limited comparative studies published, endoscopic stent placement has been associated with shorter hospital stay and lower periprocedural mortality in patients with GOO secondary to pancreatic cancer (26,27) and with more rapid food intake compared with surgical bypass (26,28). Stent placement has even been shown to be effective in palliating symptoms from obstruction in the setting of limited degrees of peritoneal carcinomatosis (29).
Delayed stent failure can occur, however, from food impaction or re-obstruction caused by tumor ingrowth. Stent migration also can occur, sometimes in association with cancer treatment, if there is reduction in the size of the tumor. In most cases, re-obstruction due to tumor ingrowth can be managed with the placement of a second stent or tumor ablation by Nd:YAG laser or argon plasma coagulator (30). In comparative studies, those managed with stent did just as well initially as patients managed with surgical bypass, but they had a greater need for re-intervention because of delayed stent occlusion (28,31).
Only gold members can continue reading. Log In or Register to continue